Downloaded 97 times
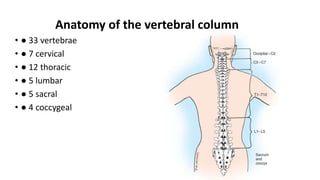
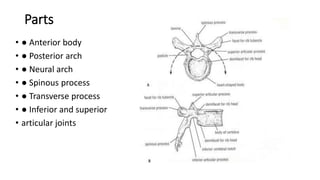
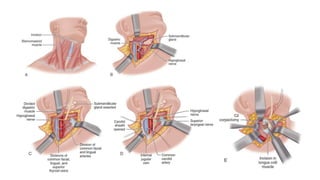
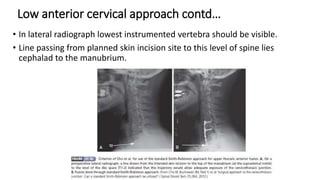
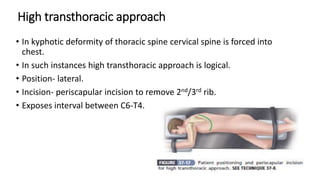
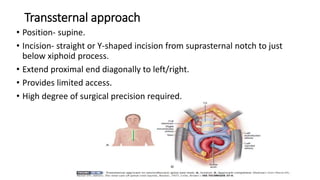
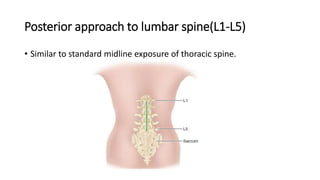
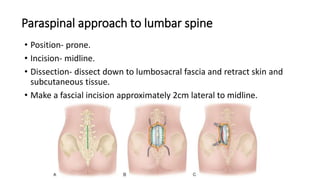
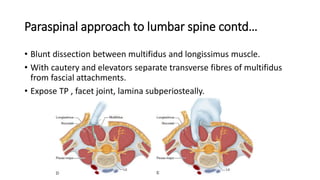


This document provides an overview of various surgical approaches to the spine, including anterior, posterior, and lateral approaches. It describes the anatomy of the vertebral column and details specific approaches for different regions of the spine, including the cervical, thoracic, lumbar, and sacral regions. Approaches discussed include the anterior retropharyngeal approach for the upper cervical spine, costotransversectomy for the thoracic spine, anterior retroperitoneal for the lumbar spine, and paraspinal for exposing the lumbar facets. Complications of different approaches are also mentioned.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












