Download as PDF, PPTX

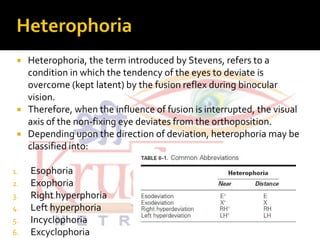


This document discusses the classification and terminology used for strabismus (eye misalignment). It defines different types of strabismus such as phoria, tropia, and heterophoria based on the presence of fusion. It also classifies strabismus based on factors like deviation direction, variation with gaze, age of onset, and etiology. Various types of strabismus deviations and causes like paralytic, mechanical, and orbital are described. References for further information on strabismus classification are provided.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










