Downloaded 49 times

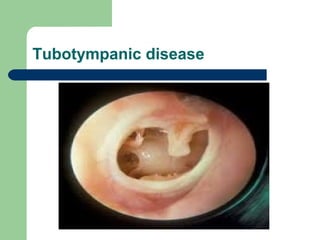
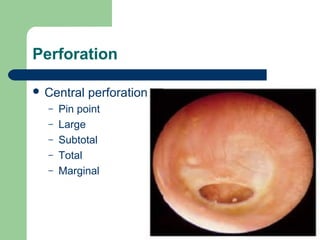


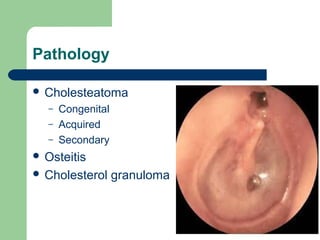
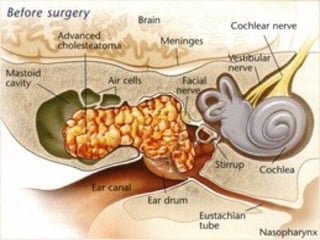
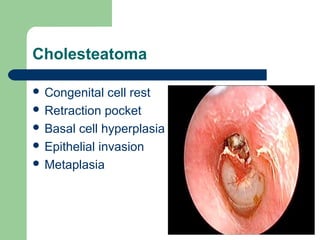





Chronic suppurative otitis media (CSOM) is a long-standing middle ear infection characterized by ear discharge and tympanic membrane perforation, with two types: tubo-tympanic (safe) and attico-antral (unsafe). Clinical features include various ear discharges and hearing loss, and treatment options involve both medical management, such as antibiotics and aural toilet, and surgical interventions like myringoplasty and mastoid exploration. Complications can arise from CSOM, including both intratemporal and intracranial issues, necessitating thorough investigation and management.


























































































