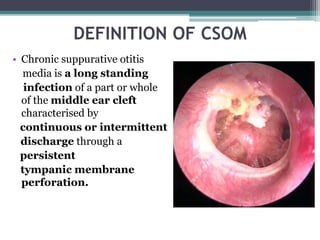
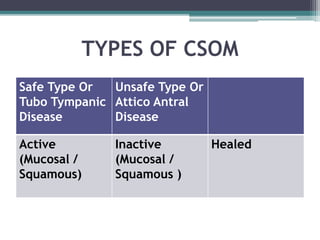
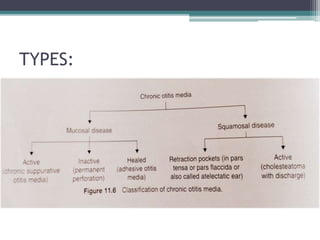
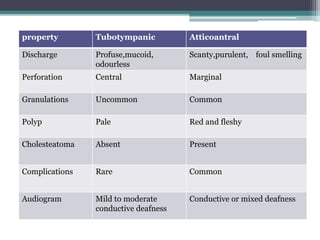
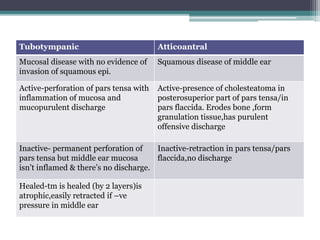
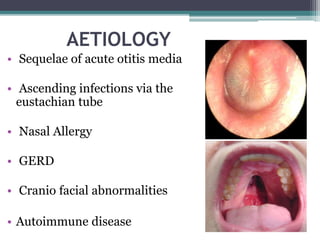
Chronic suppurative otitis media (CSOM) is a long-standing ear infection characterized by persistent ear drainage through a perforated eardrum. It is more common in developing countries and affects all ages. CSOM can be tubotympanic type, confined to the middle ear space, or atticoantral type, involving the mastoid air cells. Atticoantral disease poses greater risks of complications due to bone erosion and possible cholesteatoma formation. Treatment involves topical and oral antibiotics as well as surgical procedures like myringoplasty, tympanoplasty, and ossiculoplasty to repair damaged structures and stop drainage.