Downloaded 174 times
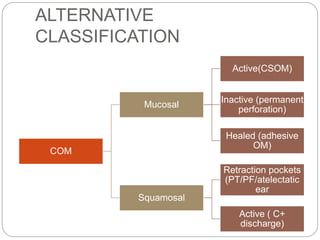

This document discusses chronic suppurative otitis media (CSOM), specifically atticoantral disease. CSOM is characterized by ear discharge and permanent perforation due to long-standing middle ear infection. Atticoantral CSOM involves the attic and antrum regions and poses a higher risk of complications due to bone-eroding processes like cholesteatoma and granulation tissue. Surgical treatment such as atticotomy or mastoidectomy aims to remove disease and render the ear safe, while reconstructive surgery seeks to preserve or restore hearing.



































































