Downloaded 52 times





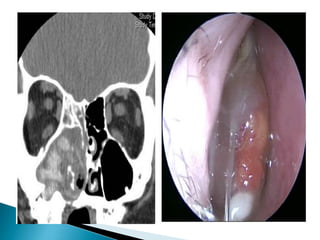


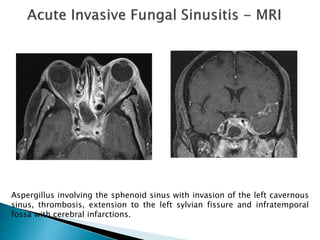
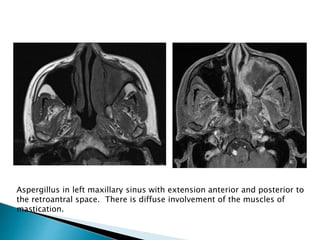
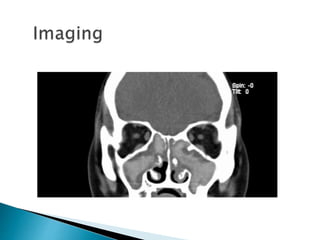
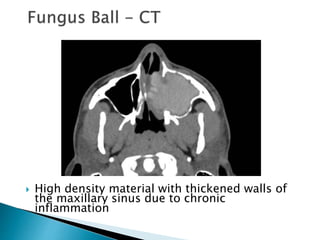




This document discusses fungal sinusitis, describing the different types including invasive, noninvasive, allergic, and chronic. Invasive fungal sinusitis is the most lethal form with mortality rates of 50-80% and usually affects immunocompromised patients. Clinical presentation varies depending on type but may include fever, facial pain, nasal congestion, and proptosis. Diagnosis involves imaging like CT and MRI to identify fungal invasion of sinus tissues and bones. Treatment requires aggressive surgical debridement and antifungal therapy along with managing any underlying immunosuppression. Prognosis depends on extent of invasion, with intracranial spread having the highest mortality.

















































































