Downloaded 14 times
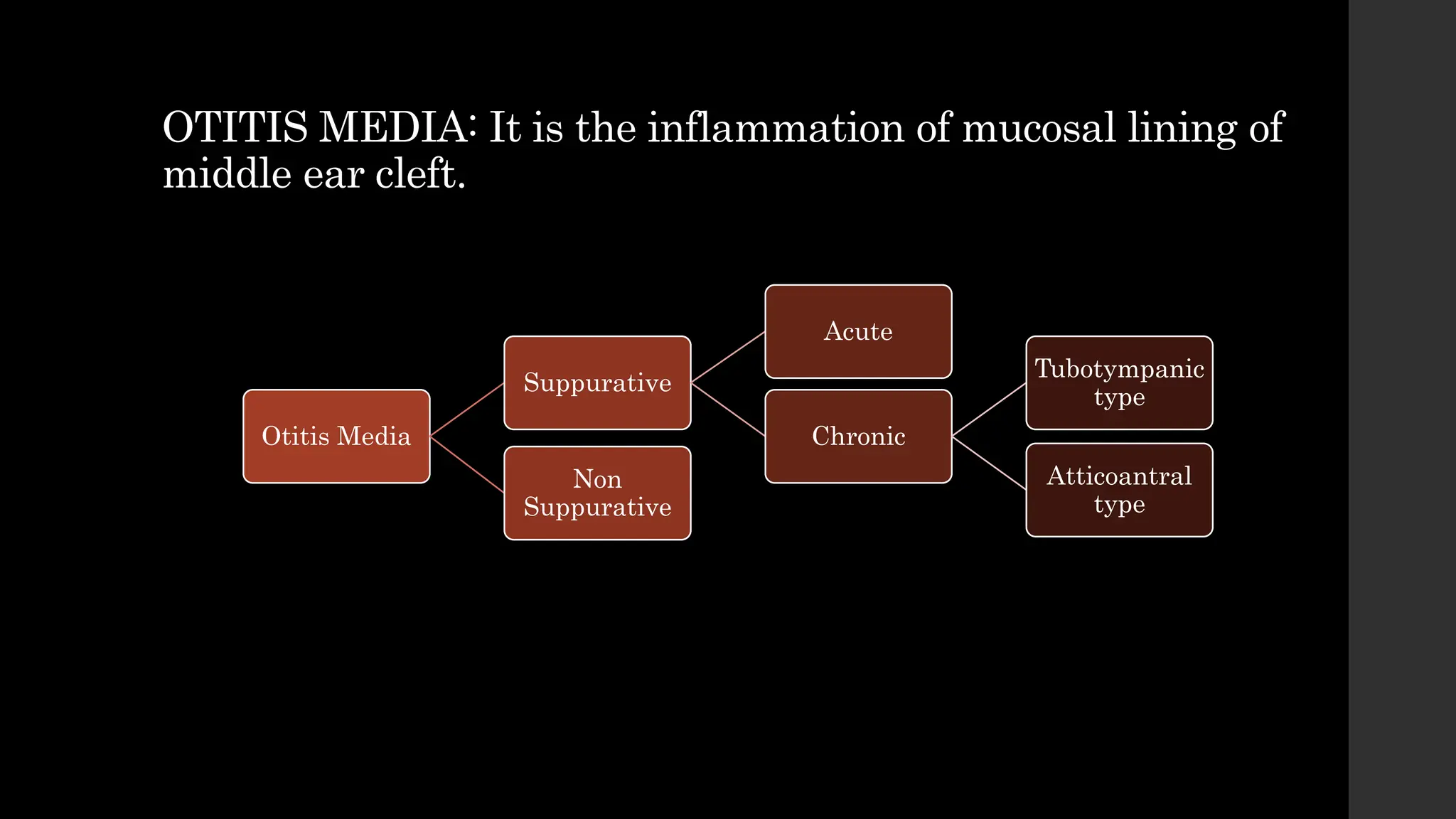



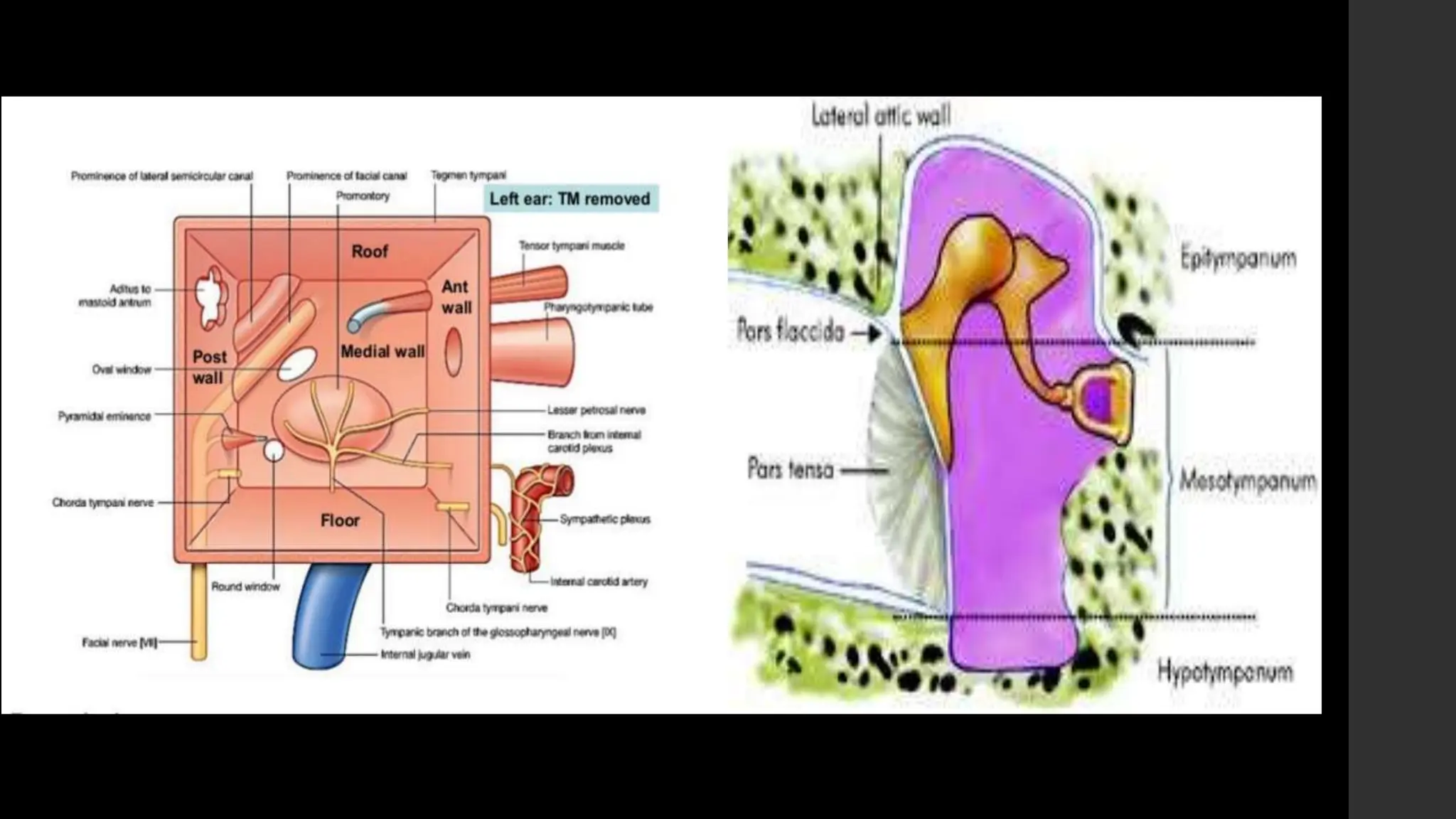














Chronic suppurative otitis media (CSOM) is an infection of the middle ear characterized by ear discharge through a perforated eardrum for more than 3 months. It is caused by acute otitis media or middle ear effusions and is more common in developing countries. CSOM can be tubotympanic type, involving the front part of the middle ear, or atticoantral type, involving the back part and often associated with cholesteatoma. Treatment involves cleaning the ear, antibiotic ear drops, surgery to repair the eardrum or remove disease, and addressing underlying causes.



































































