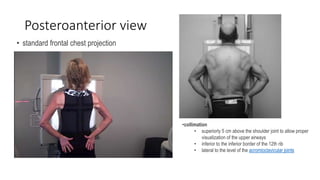
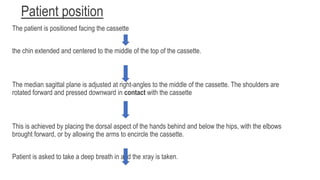
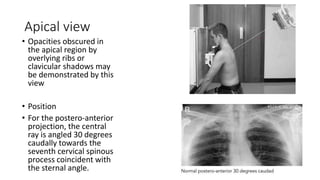
Chest radiography involves several standard views and positions to properly visualize the lungs and chest. The posteroanterior view is standard and involves the patient standing facing the cassette with chin extended. Additional views include lateral, lateral decubitus, lordotic, and oblique views which provide different angles. Proper inspiration, penetration, and no rotation are important for technical quality. Positioning varies slightly for anteroposterior supine views and between views, but consistently aims to properly center and collimate the chest within the beam and cassette.


















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










