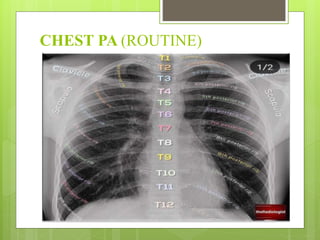
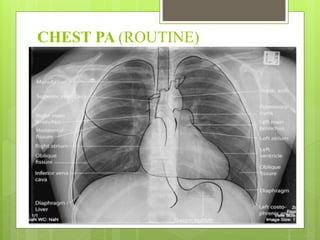
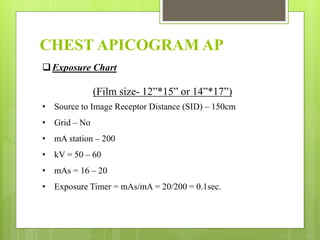
The document details the various types of chest radiography, including routine and special views, and provides guidance on patient positioning, exposure settings, and the clinical applications of each view, such as diagnosing conditions like pneumonia and pleural effusion. It also includes specific measurements for the cardiothoracic ratio (CTR) and elaborates on the use of different projections like PA, lateral, and oblique views. Comprehensive charts outline exposure parameters for each view to ensure accurate imaging and diagnostics.
![Cardio – Thoracic Ratio (CTR)
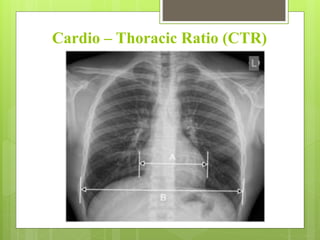
The method of determining the CTR –
The cardiothoracic ratio is measured on only a PA chest x-ray.
The CTR is determined on the basis of the ratio of the transverse heart
dimension [A] to the transverse dimension of the chest (internal ribs) [B]
measured on the radiograph in the chest PA projection: CTR = A/B.
A normal measurement is 0.42-0.50.
A CTR > 0.5 (or > 50%) is considered abnormal. In radiology reports, terms
like “cardiomegaly” or “increased heart size” are commonly used to describe
an increased CTR.
A small cardiothoracic ratio (CTR) is defined as <42%/0.42 when assessed on a
PA chest radiograph, and is often called small heart syndrome. A
pathologically-small heart is also known as microcardia. It can be due
to/associated with a number of entities: adrenal insufficiency, e.g. Addison
disease.](https://image.slidesharecdn.com/chestradiographyppt-1-230331152551-bfabf873/85/CHEST-RADIOGRAPHY-Routine-special-radiographs-17-320.jpg)

























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











