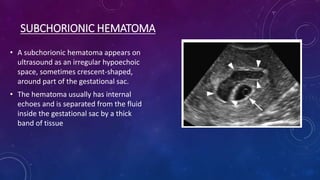
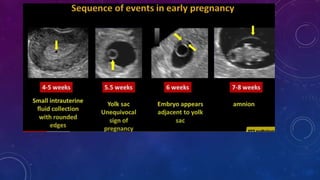
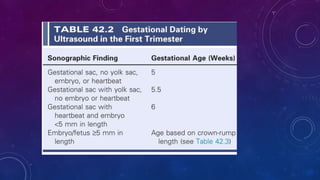
This document provides guidelines for an early ultrasound exam including indications, patient history, structures to visualize, and sonographic timeline. It details how to estimate gestational age from 5-6 weeks by measuring the mean sac diameter or identifying gestational sac contents. From 6 weeks until the end of the first trimester, gestational age correlates with the crown-rump length of the embryo or fetus. The document also provides guidelines on evaluating heart rate, yolk sac size, and identifying subchorionic hematomas.