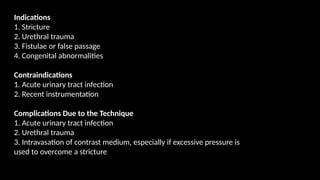
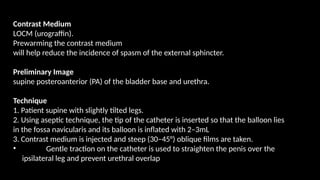
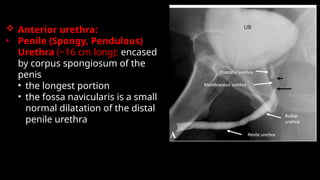
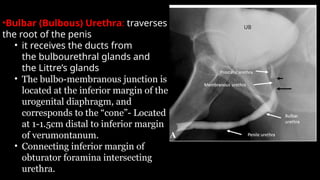
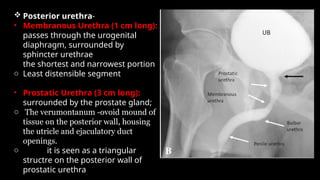
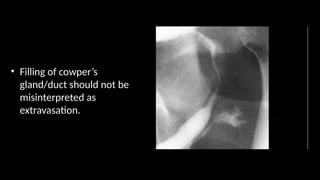
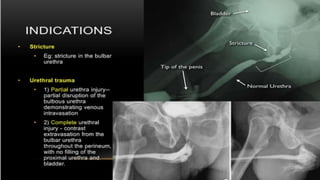
This document outlines the indications and contraindications for imaging urethra using augment imaging techniques, detailing conditions such as strictures and congenital abnormalities, while noting contraindications like acute urinary tract infections. It describes the imaging technique, including patient positioning and catheter insertion, along with specific anatomical features of the anterior and posterior urethra. Potential complications during the procedure, such as urethral trauma and contrast medium intravasation, are also mentioned.