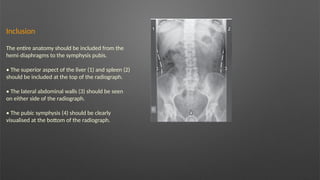
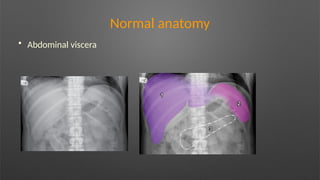
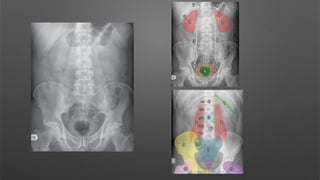
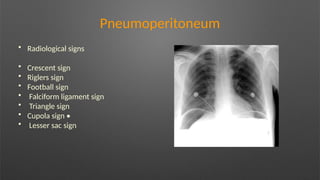
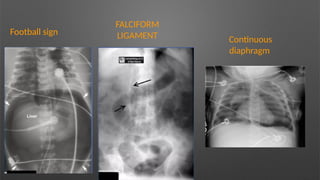
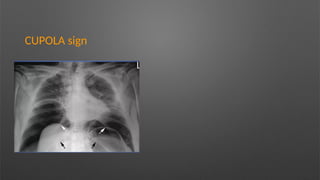
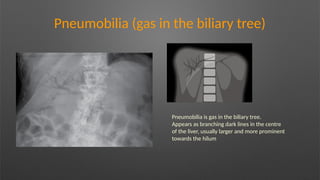
The document outlines the indications and views for plain abdominal X-rays, which are crucial for identifying conditions like bowel obstructions, perforations, and foreign bodies. It details normal anatomy and common radiological signs, as well as the expected appearances of various abdominal structures on X-rays. Additionally, it describes specific conditions that may be detected, such as air in the biliary tree and manifestations of bowel inflammation.















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















