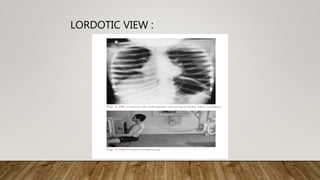
This document provides an overview of a normal chest x-ray examination. It discusses the major views used in chest x-rays including posteroanterior, anteroposterior, lateral, and lateral decubitus. It also covers technical aspects such as inspiration level, penetration, and patient rotation. Finally, it outlines the systematic approach used to analyze chest x-rays, including examining the trachea, hila, mediastinum, heart, lungs, pleura, diaphragm, bones, and soft tissues.