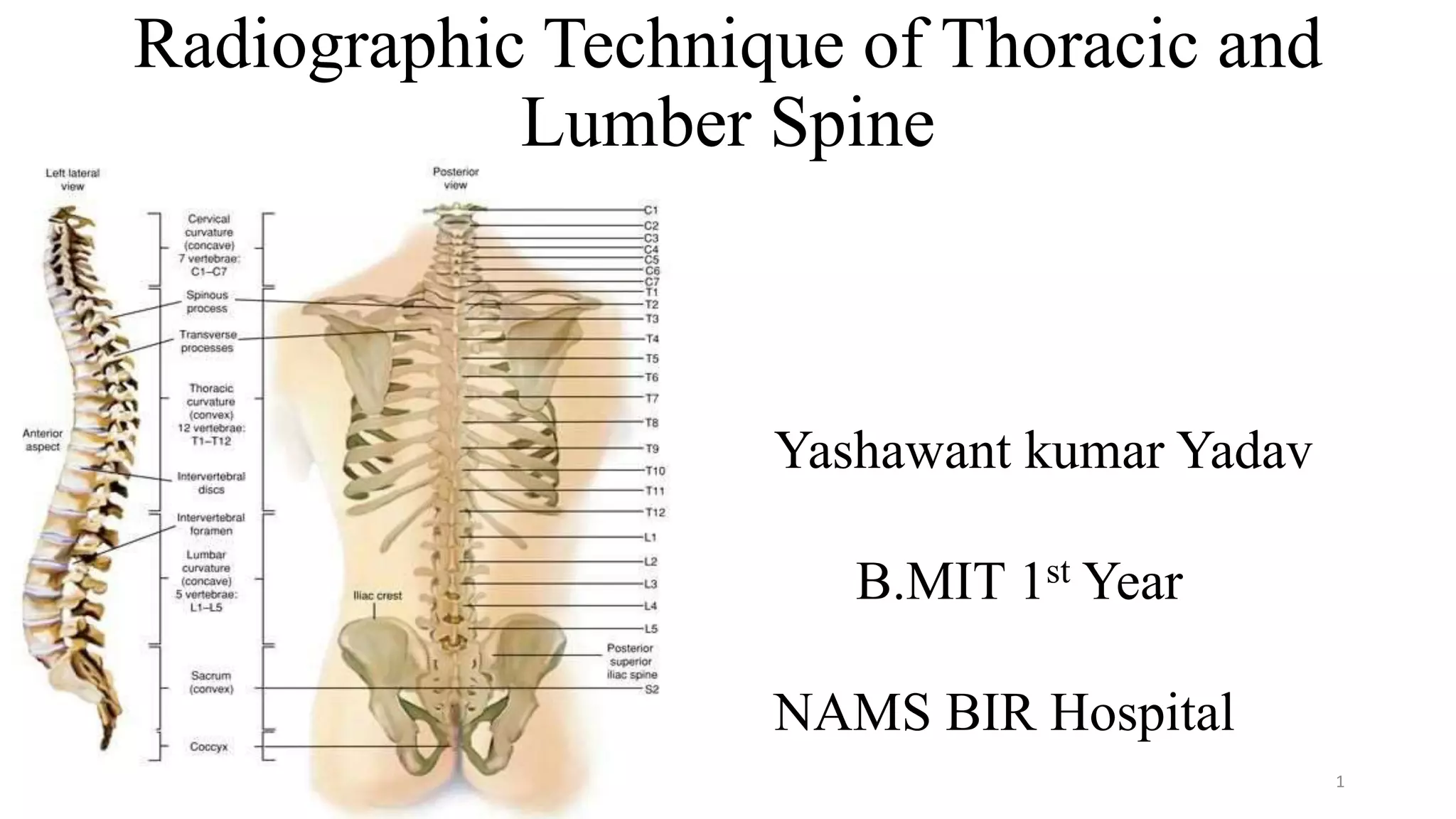
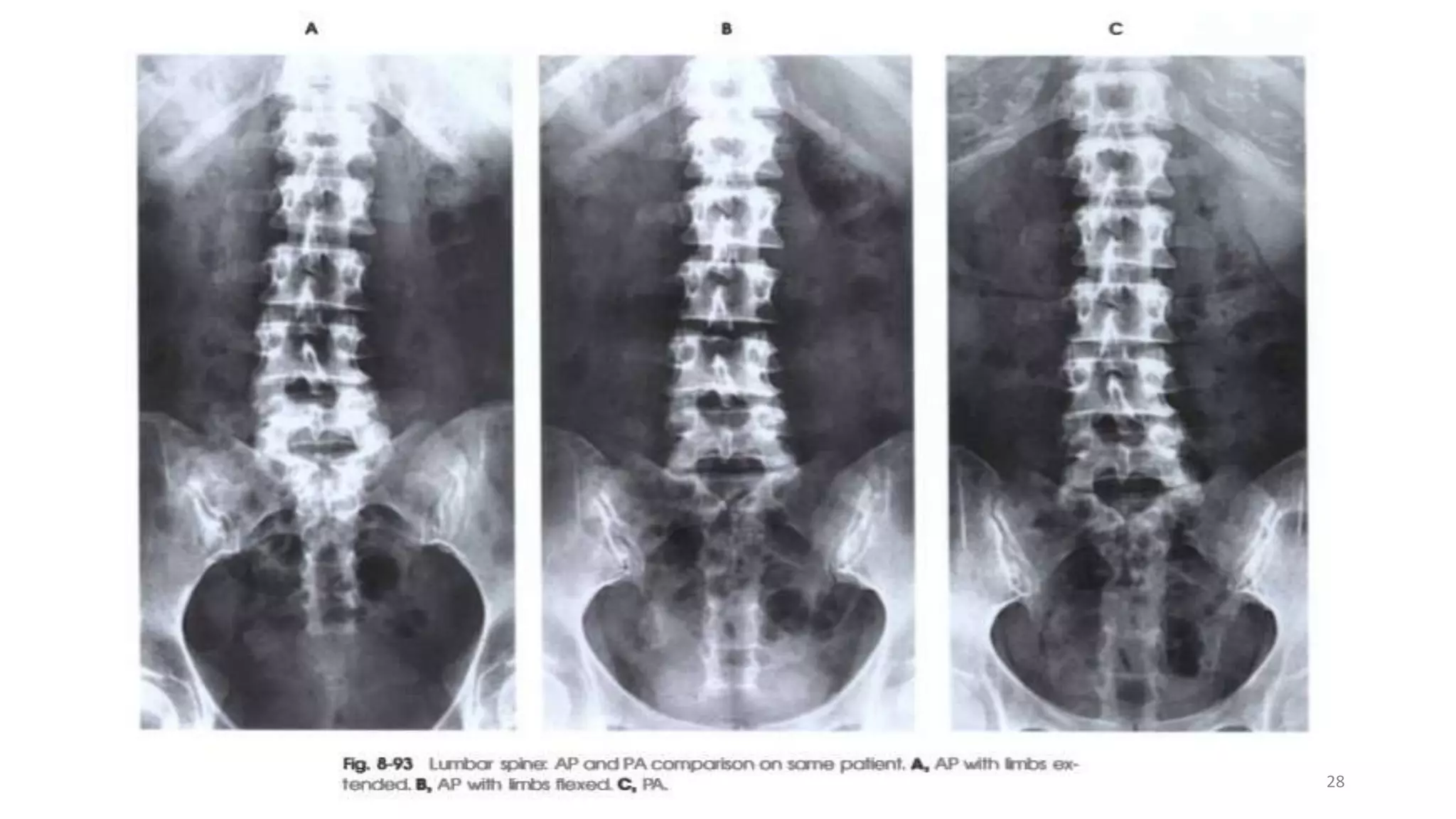
The document provides an overview of radiographic techniques for imaging the thoracic and lumbar spine. It discusses the anatomy of the thoracic and lumbar spine and provides details on positioning, centering, and essential criteria for various projections including AP, lateral, and oblique views of both the thoracic and lumbar spine. The techniques are described for common indications like trauma, fractures, and degenerative conditions.


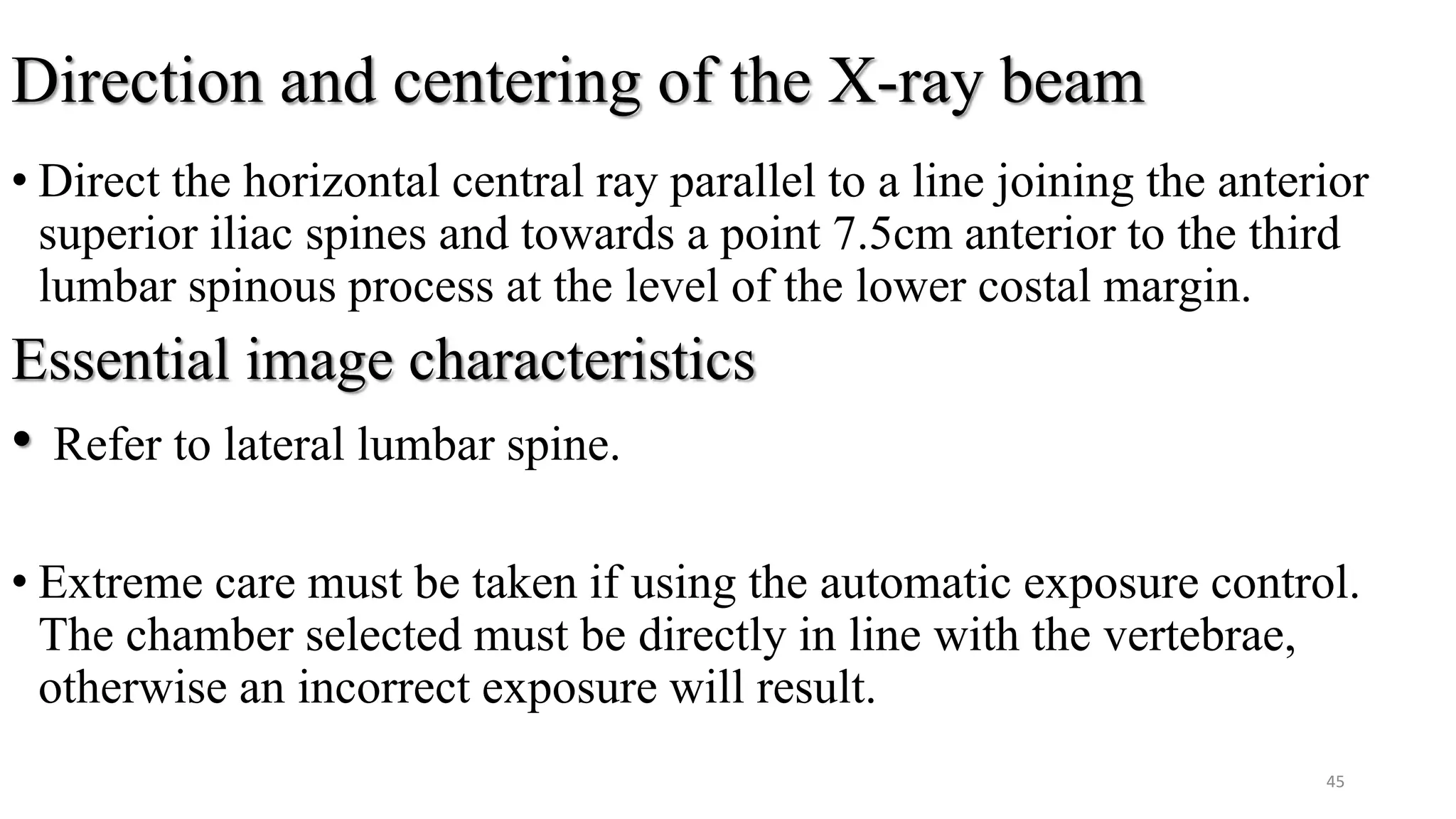
![Central ray
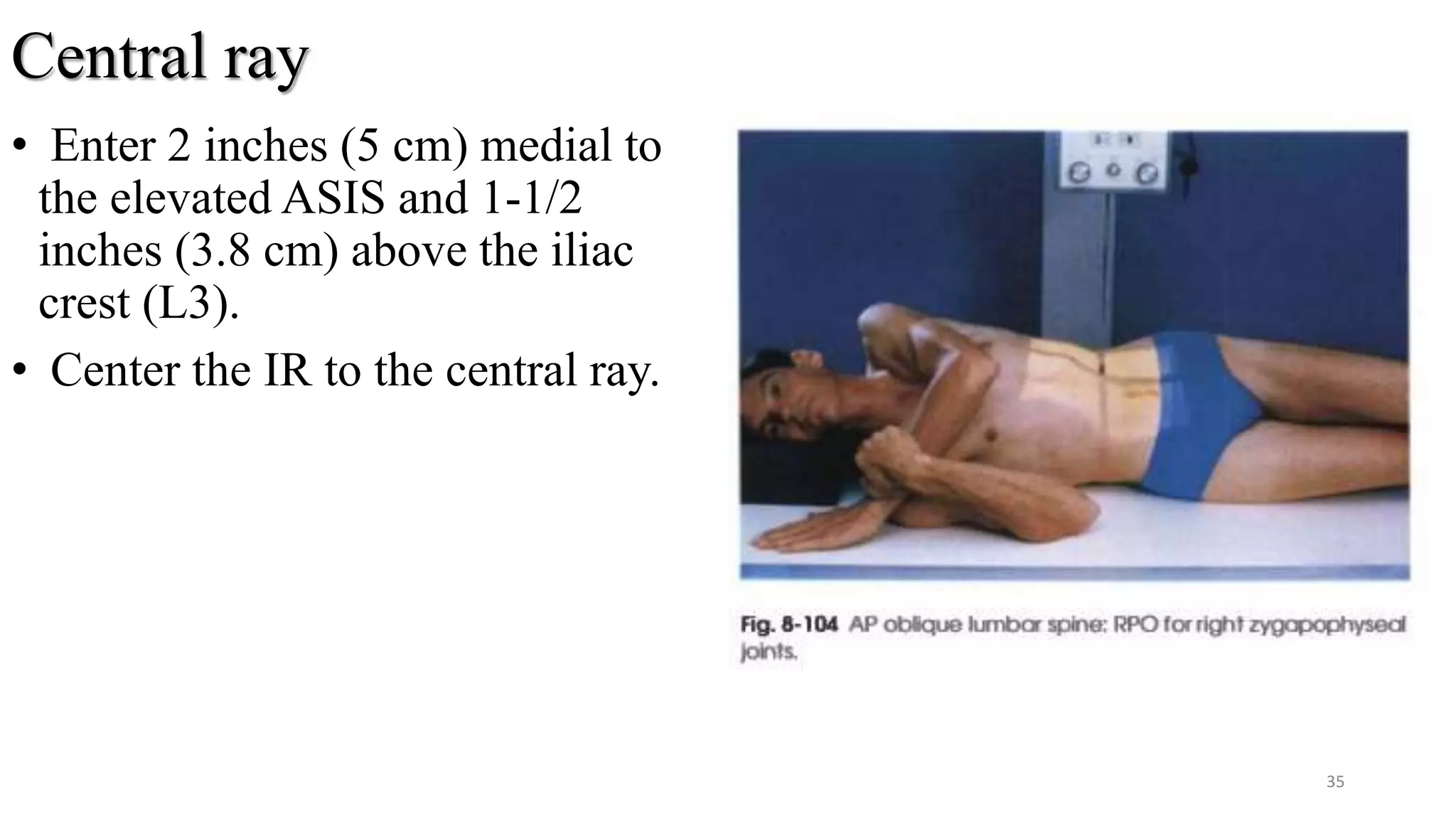
• Perpendicular to enter the L3 (1
to ½ inches [2.5 to 3.8 cm]
above the crest of the ilium).
The central ray enter the
elevated ide approximately 2
inches (5 cm) lateral to the
palpable spinous process.
39](https://image.slidesharecdn.com/presentation1-190620160842/75/Presentation1-pptx-thoraccic-and-lumber-spine-39-2048.jpg)