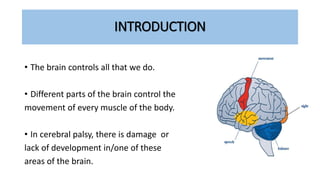






1. Cerebral palsy is a motor dysfunction caused by damage to the brain's motor areas, resulting in problems with muscle control and movement. 2. The most common type is spastic cerebral palsy, which causes muscle stiffness. Other types include dyskinetic, ataxic, and mixed forms. 3. Risk factors include prematurity, low birth weight, genetic disorders, infections, and complications during birth. Treatment involves a multidisciplinary approach including physical therapy, medications, surgery, and rehabilitation.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




