Downloaded 219 times





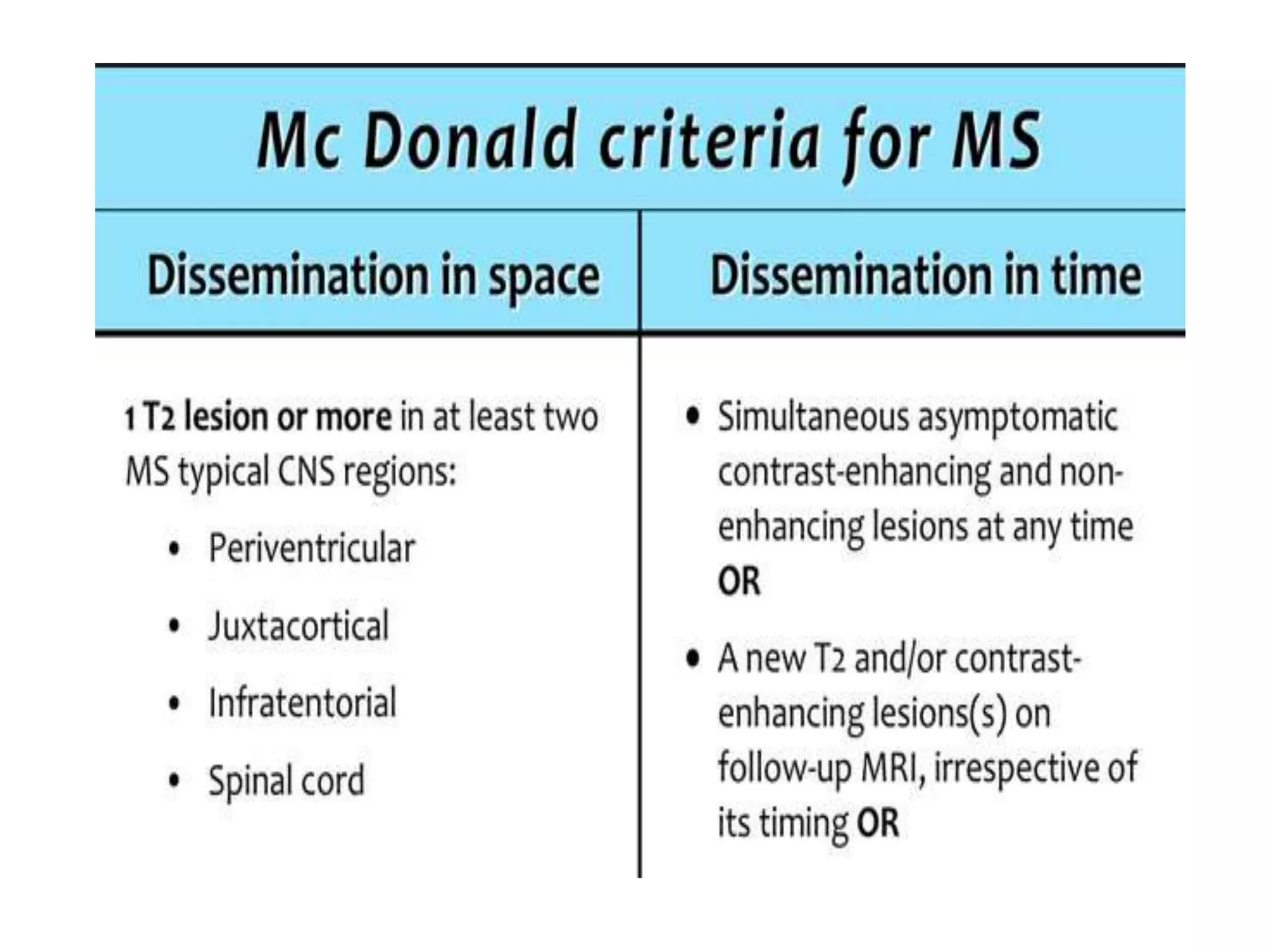
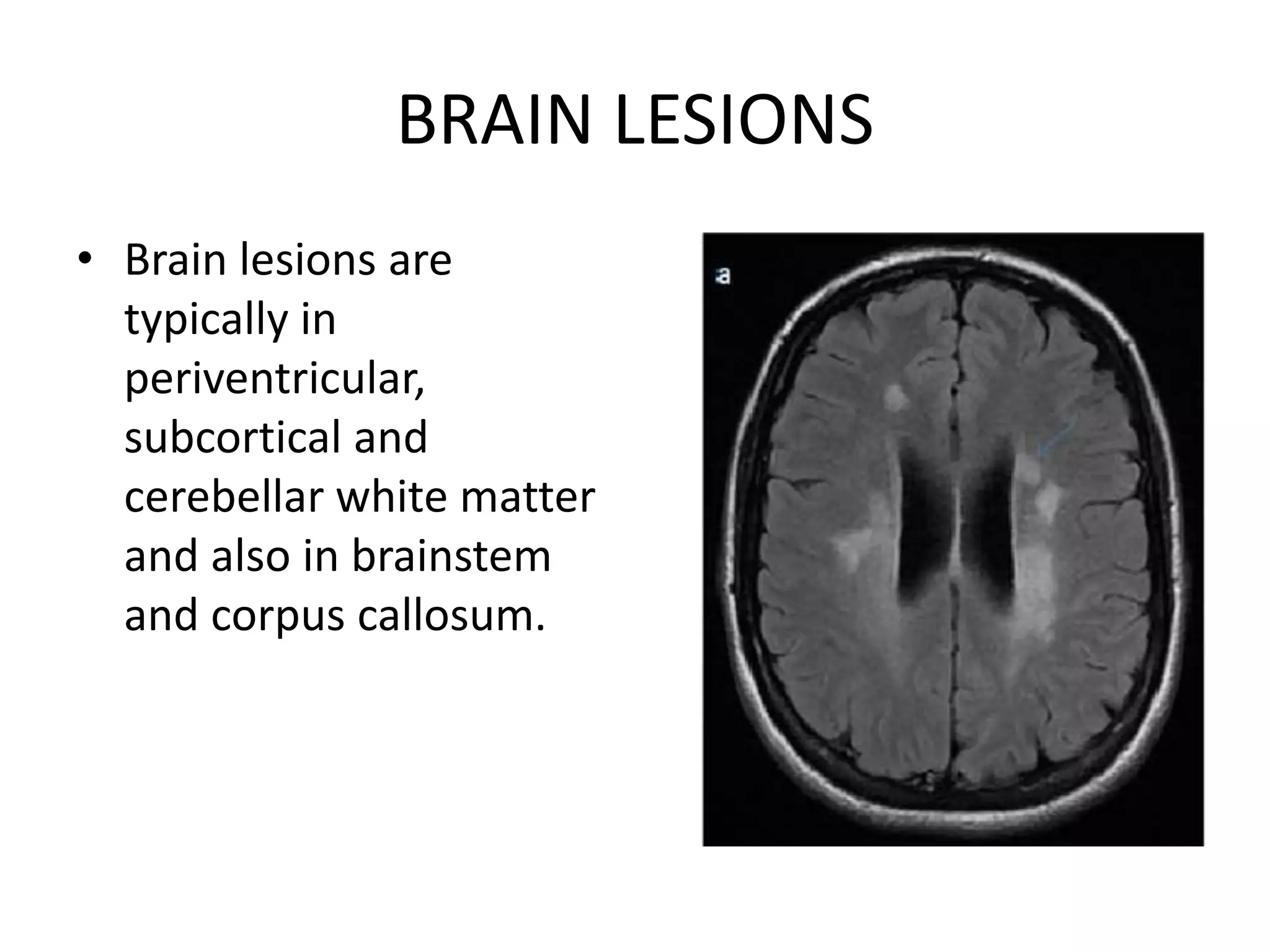






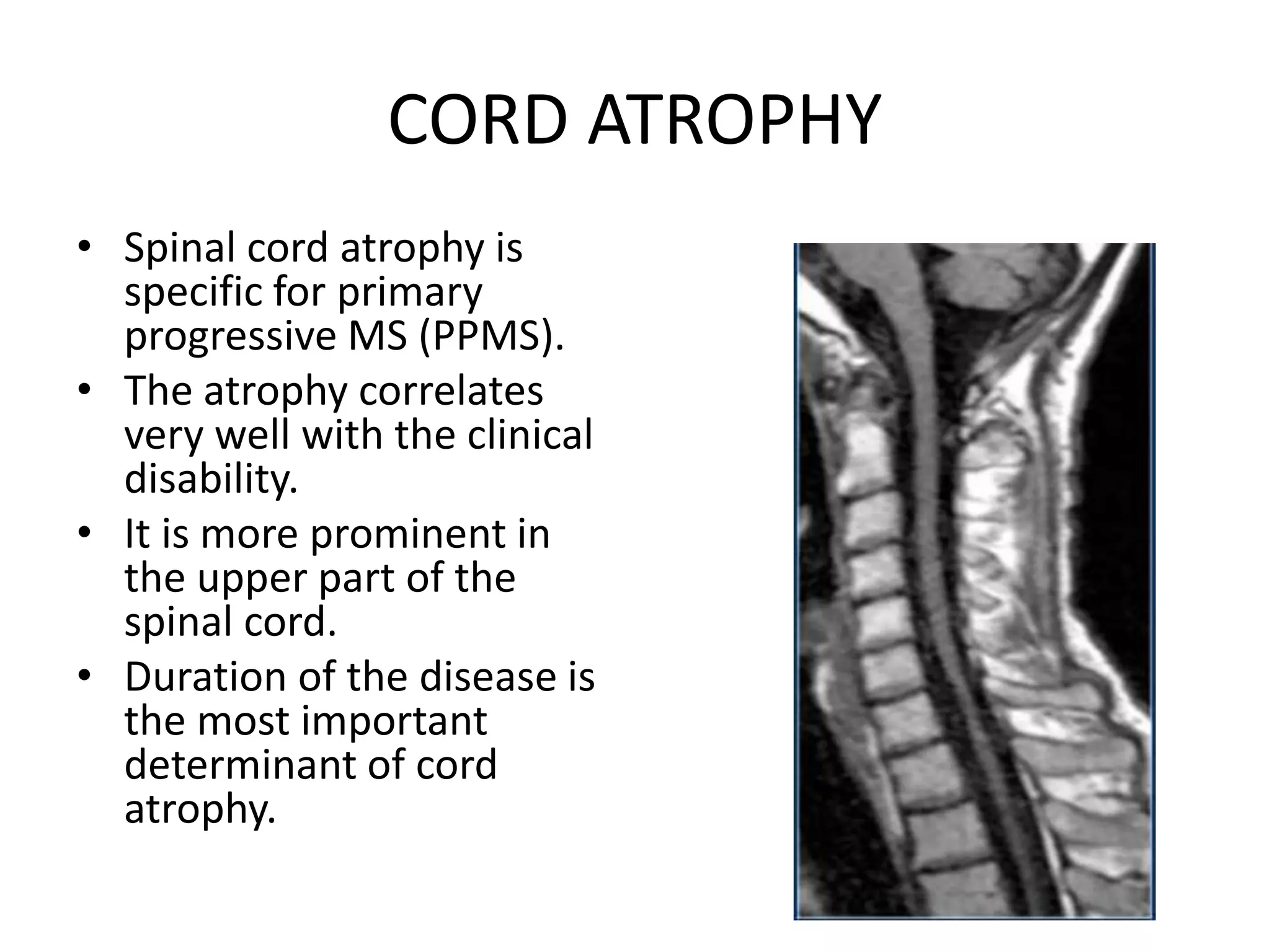



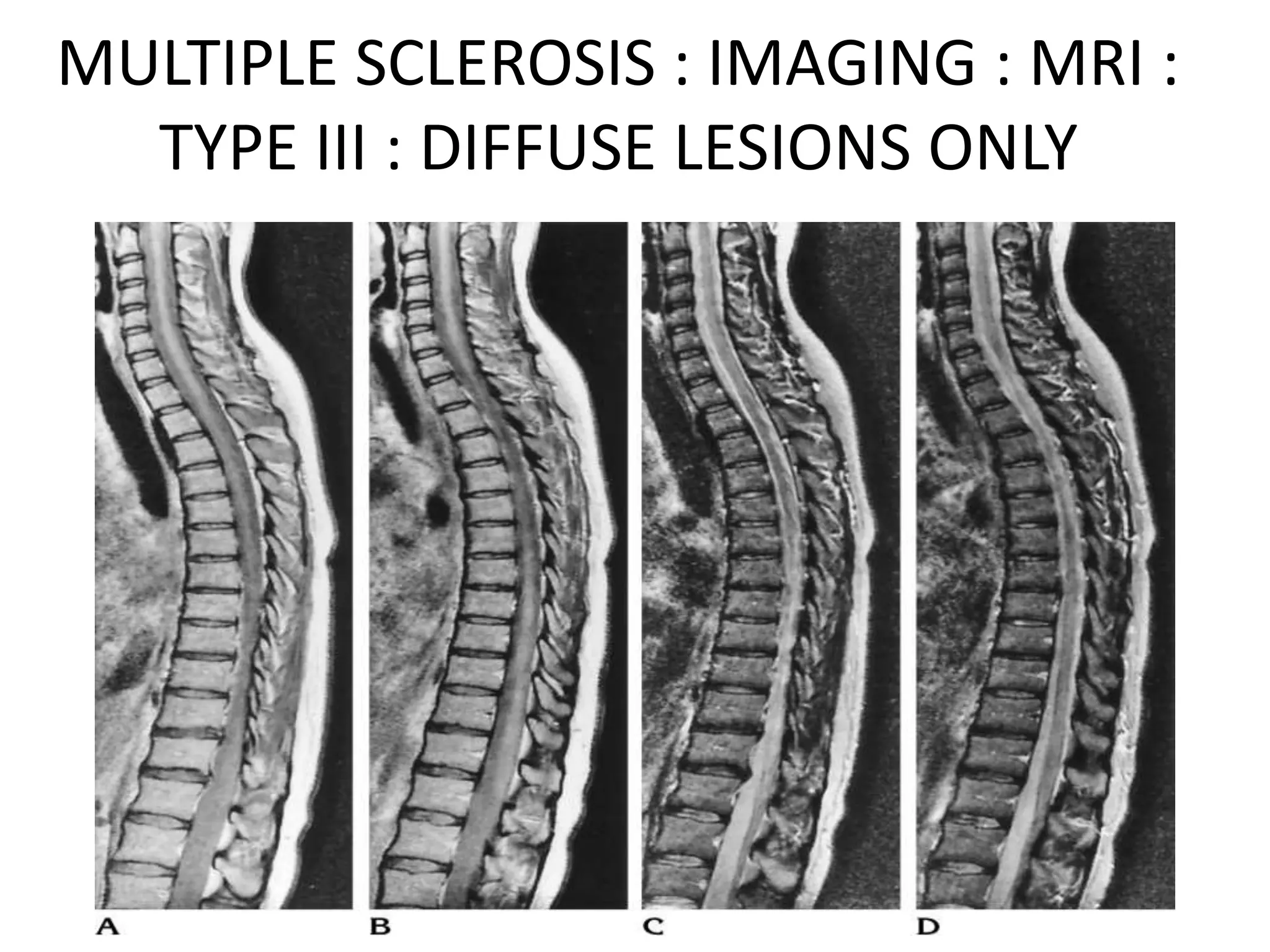













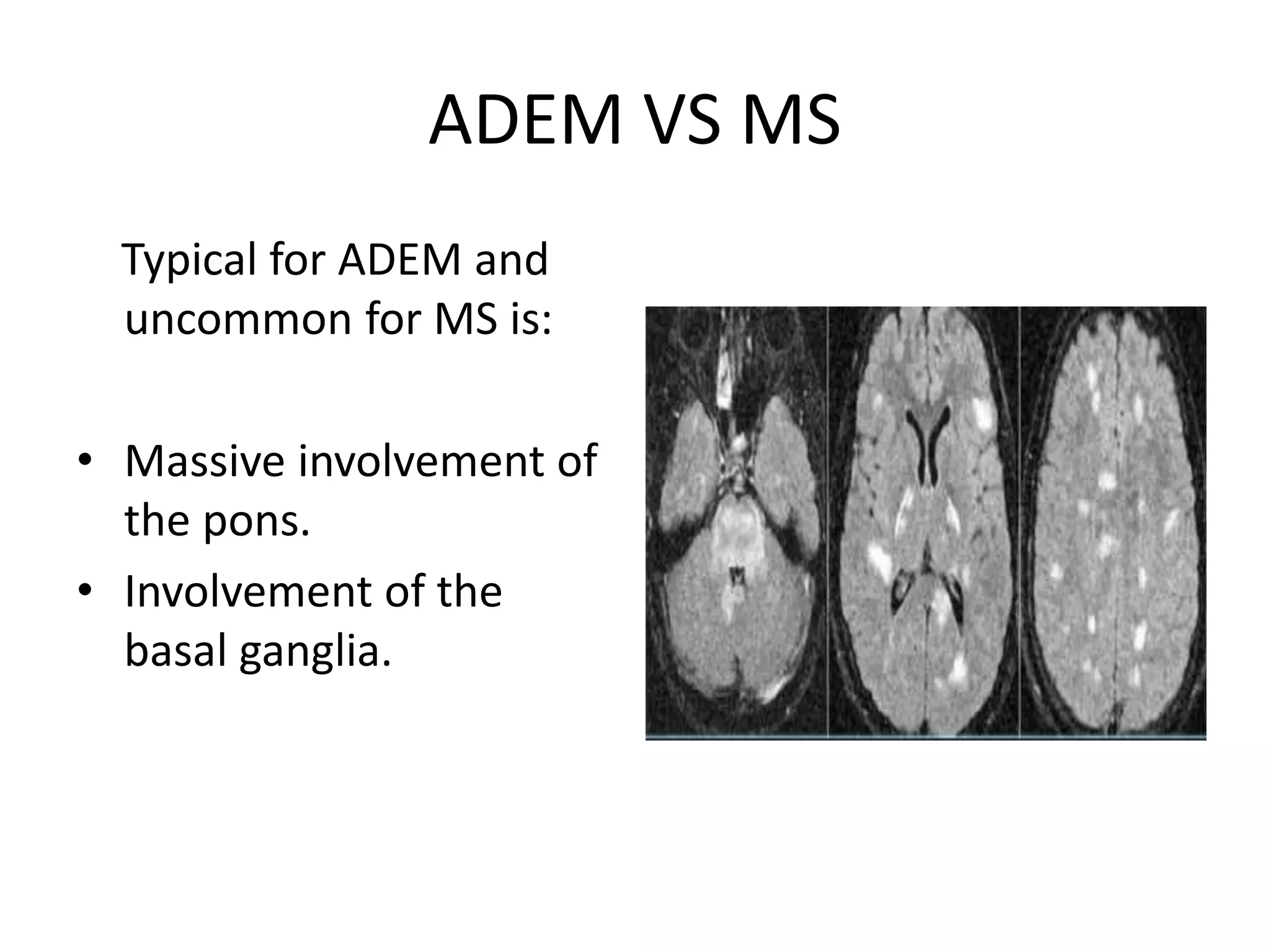







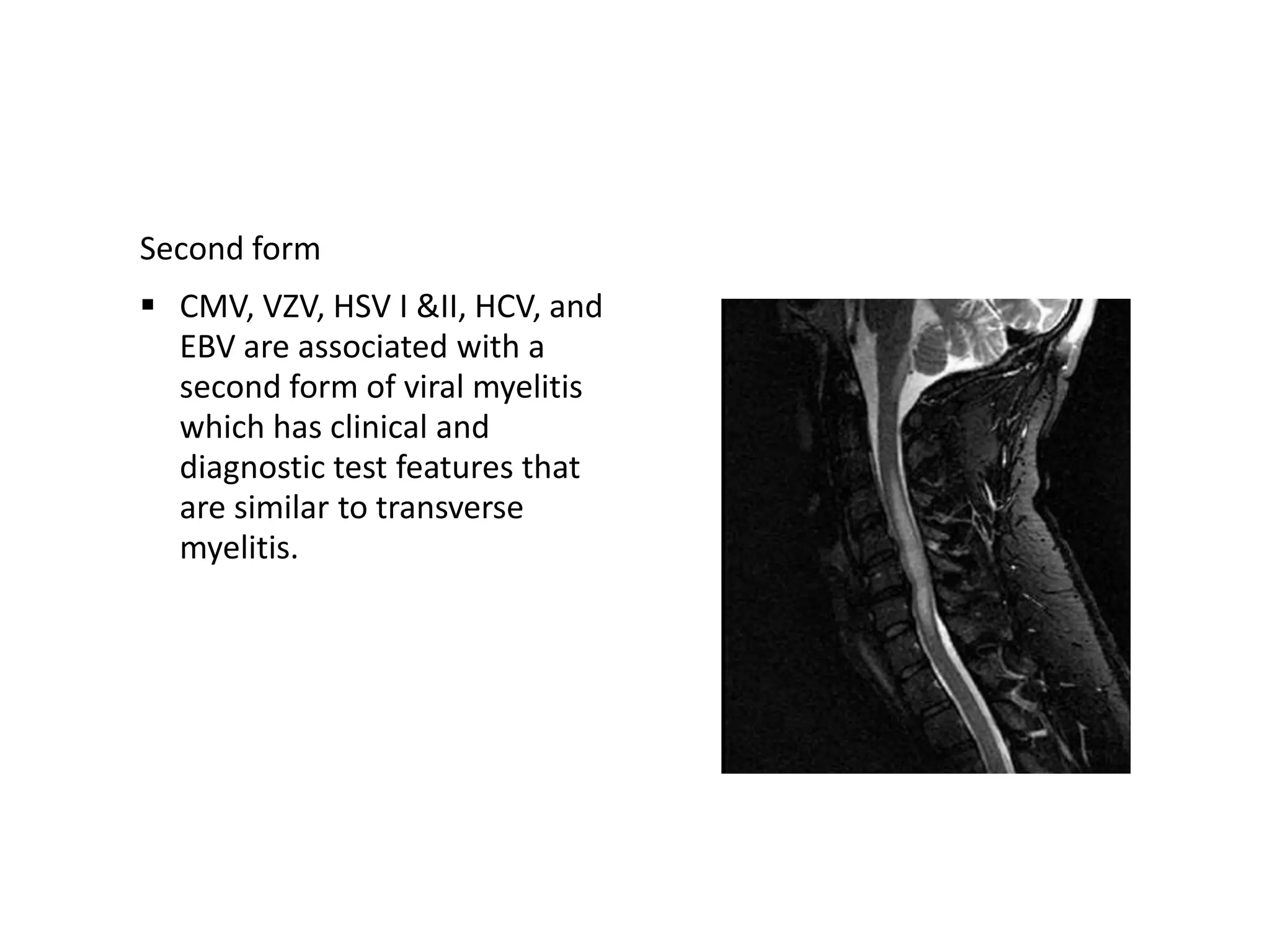












The document discusses various types of acute myelopathies affecting the spinal cord, categorizing them into compressive and non-compressive myelopathies, with detailed descriptions of conditions such as multiple sclerosis, neuromyelitis optica, acute disseminated encephalomyelitis, and others. It outlines diagnostic approaches, imaging findings, and clinical features associated with these myelopathies, emphasizing the significance of understanding symptoms and MRI characteristics for accurate diagnosis. The document also highlights key differences between conditions and the impact of inflammatory and vascular factors on spinal cord health.




































![APPROACH TO NON COMPRESSIVE MYELOPATHY [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtononcompressivemyelopathyautosaved-240930073343-8621cff7-thumbnail.jpg?width=640&height=640&fit=bounds)














































