Downloaded 60 times



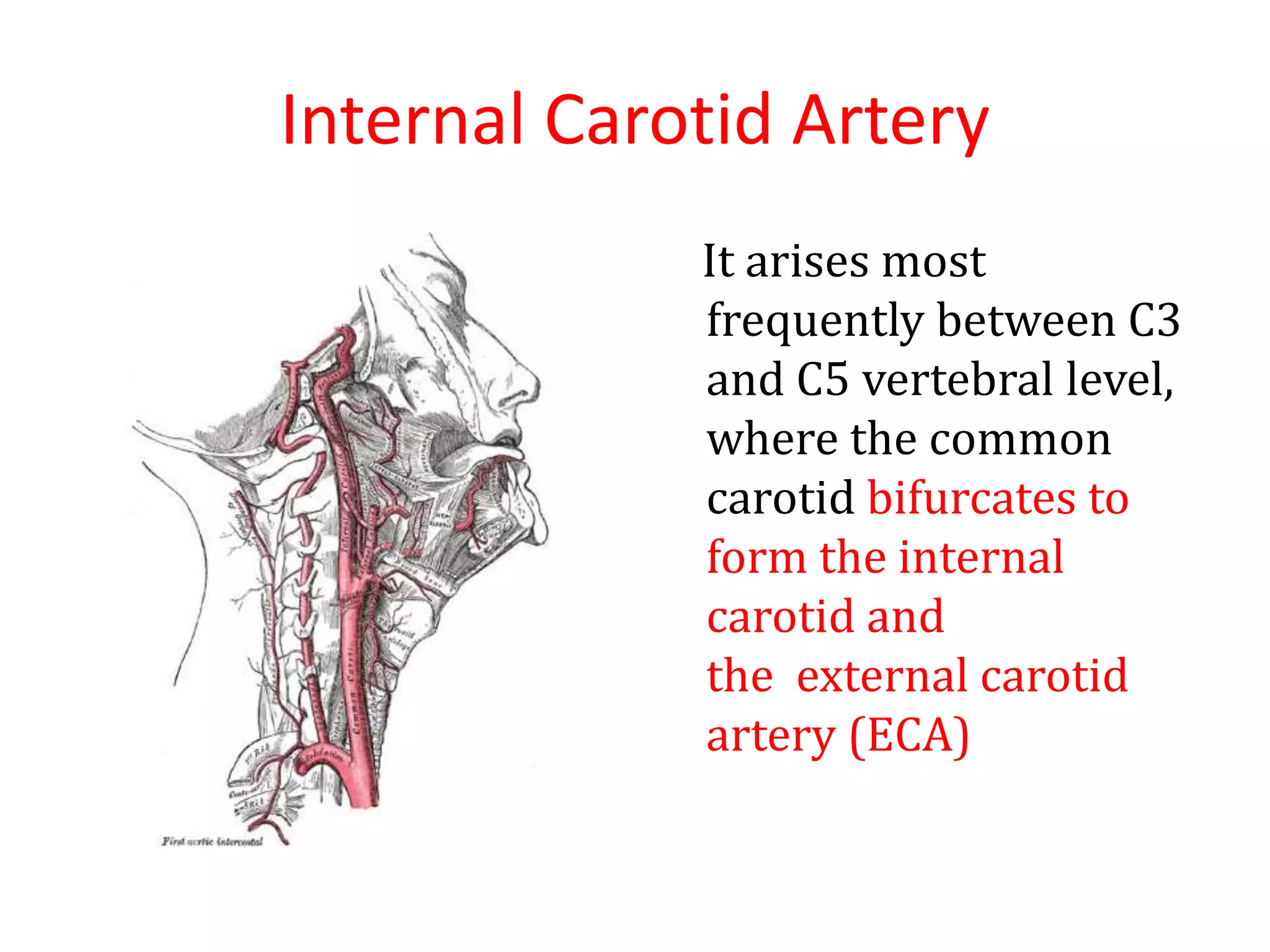

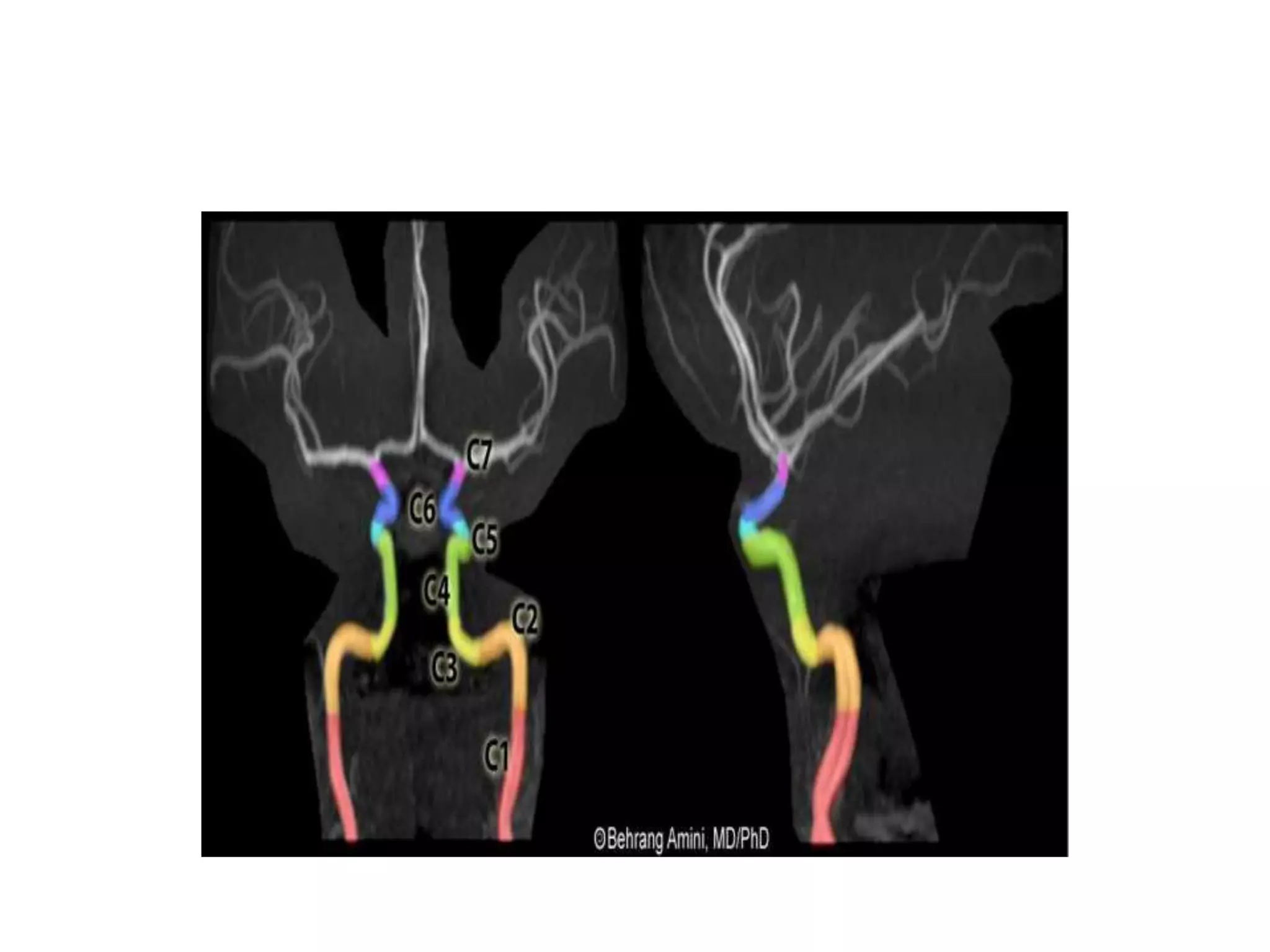
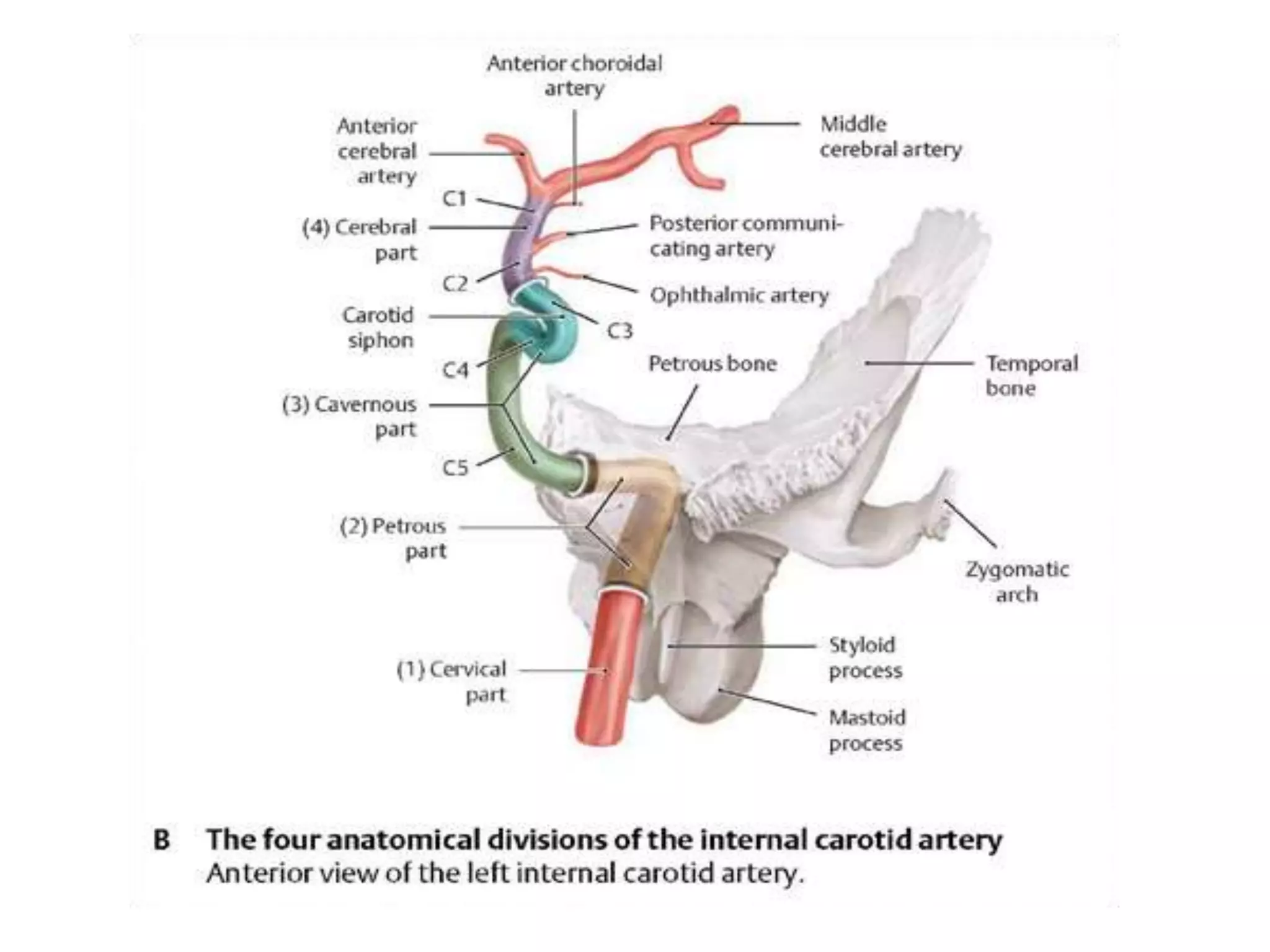


























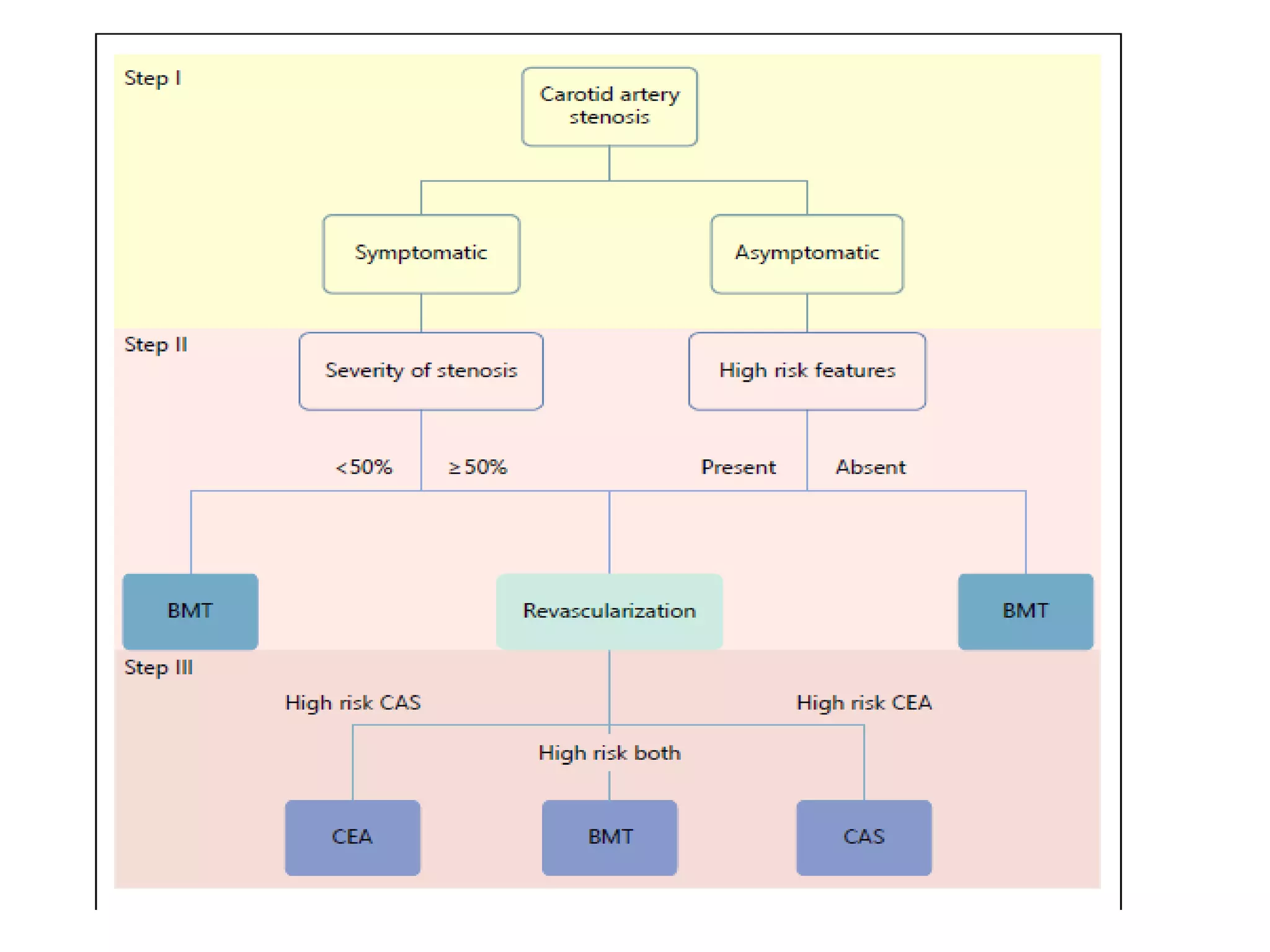






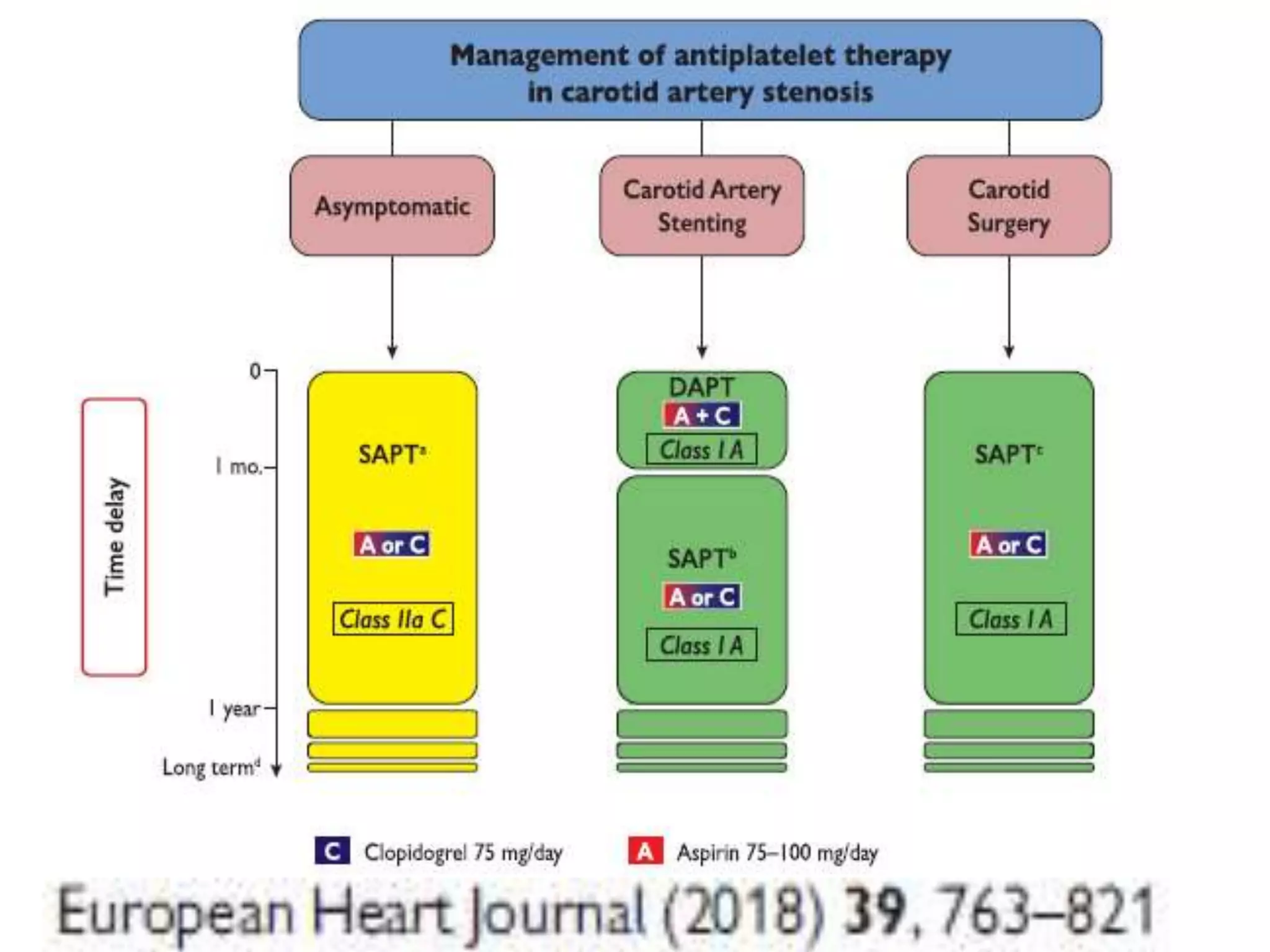
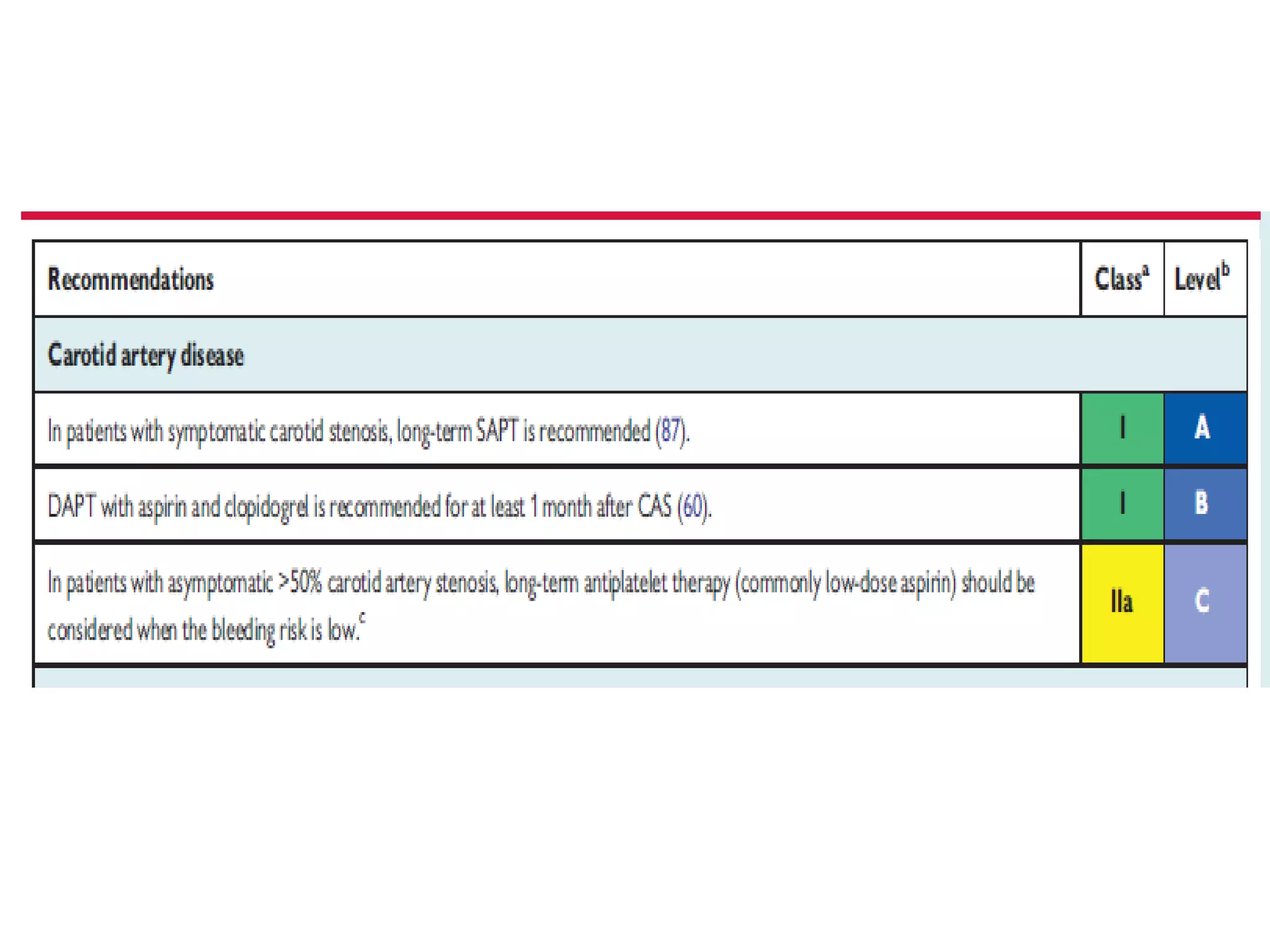
































Carotid artery stenosis refers to a 50% or greater blockage of the carotid arteries, which supply blood to the brain. The document discusses the anatomy of the carotid arteries and risk factors for ischemic stroke such as atherosclerosis. For asymptomatic patients, screening with carotid duplex ultrasound may be considered for those with multiple cardiovascular risk factors. Medical management including statins, blood pressure control, and aspirin can significantly reduce stroke risk. For high-risk asymptomatic patients, carotid endarterectomy or stenting may be options. Symptomatic patients with greater than 50% stenosis are generally treated with carotid revascularization, especially if additional risk factors are present.



































































