

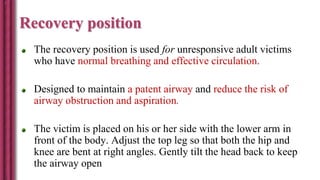
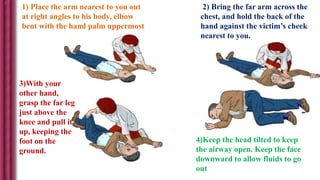
![ENSURE SAFETY
Safety Of Self
Safety Of client
Movement of a trauma victim – only when absolutely
necessary
[unstable cervical spine – injured spinal cord]
Make sure the environment is safe for rescuers and victim](https://image.slidesharecdn.com/cardiopulmonaryresuscitationbls-160630102132/85/Cardio-pulmonary-resuscitation-BLS-20-320.jpg)


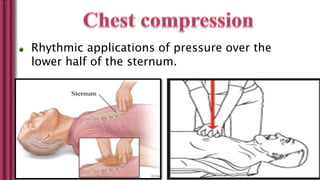





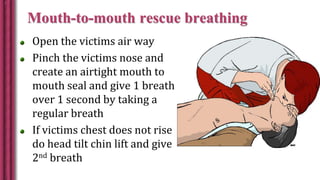
![Rescue breathing
During CPR , C.O. is 25 – 33% of normal so oxygen
uptake from the lungs and CO2 delivery to the lungs are
also reduced.
Tidal vol : 6-7 ml/kg = 500-600 ml [ 1-2 L bag]
Risk of:
-Reduced venous return to heart.
-Gastric inflation – regurgitation , aspiration, splinting of lung
by diaphragm.](https://image.slidesharecdn.com/cardiopulmonaryresuscitationbls-160630102132/85/Cardio-pulmonary-resuscitation-BLS-52-320.jpg)

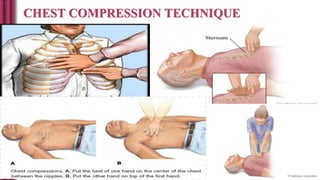
Cardiopulmonary resuscitation (CPR) is an emergency procedure used when a person's heart has stopped beating and breathing has stopped. It involves chest compressions and rescue breathing to maintain circulation and oxygenation until medical help arrives. Basic life support (BLS) involves chest compressions, opening the airway, and rescue breathing without any equipment other than a face mask or shield. BLS aims to maintain circulation and oxygenation through chest compressions and rescue breathing until advanced life support can take over. Proper CPR technique is critical to maximize its effectiveness in saving lives.




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




