

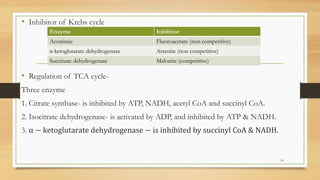

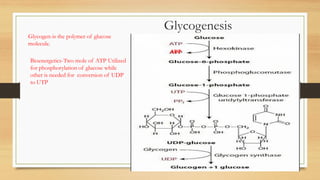
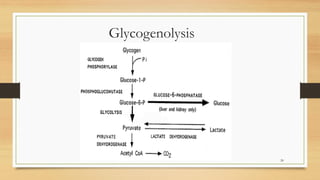
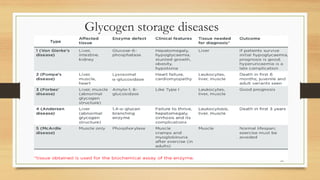







The document provides an extensive overview of carbohydrate metabolism, including key pathways such as glycolysis, the citric acid cycle, gluconeogenesis, glycogen metabolism, and the hexose monophosphate shunt. It details the biochemical processes involved, the significance of each pathway, and their roles in energy production and metabolic regulation, while also mentioning the effects of hormonal influences on carbohydrate metabolism. Additionally, it addresses conditions like G6PD deficiency and discusses implications for blood glucose regulation and diabetes mellitus.












































![Carbohydrate metabolism final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/carbohydratemetabolismfinalautosaved-250929151656-3b0eb421-thumbnail.jpg?width=640&height=640&fit=bounds)




























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













