Downloaded 1,062 times



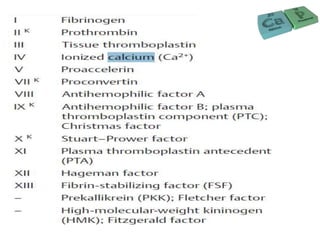
![BONE SALTS
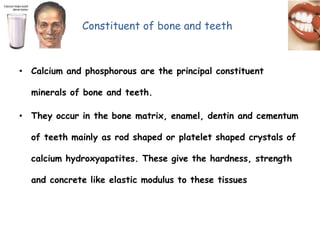
The crystalline salts deposited in the organic matrix of bone are
composed principally of calcium and phosphate.
The major crystalline salt is known as hydroxyapatite
[Ca10(PO4)6(OH)2].](https://image.slidesharecdn.com/7umig7cnrjqrw2wzpdrx-signature-7d026324264c1f55cdf36b88e78788580efb936718fbd8ad397e573d70e66131-poli-160402122754/85/Calcium-and-phosphate-METABOLISM-35-320.jpg)


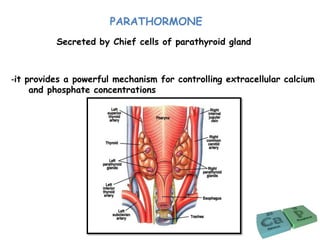
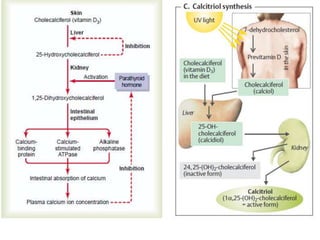
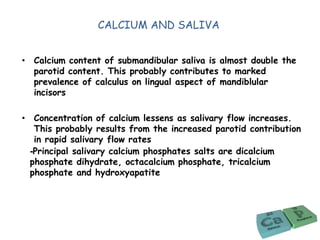

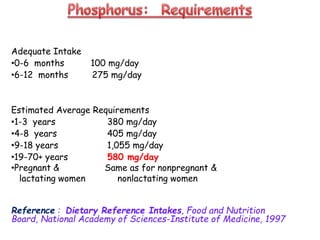
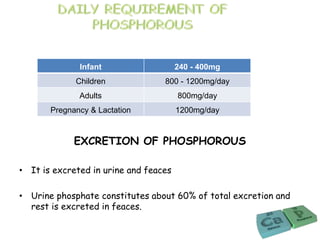
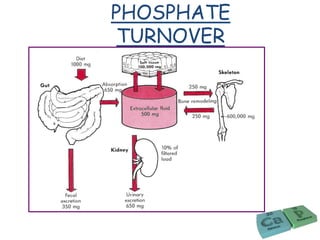
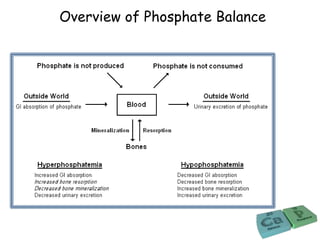




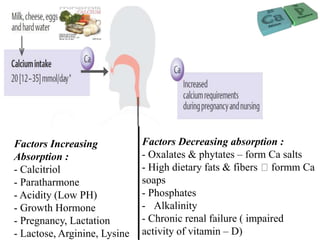
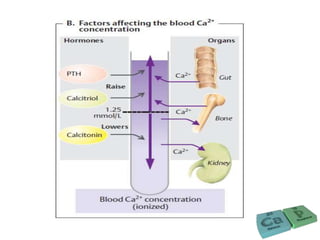
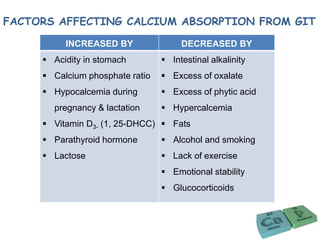
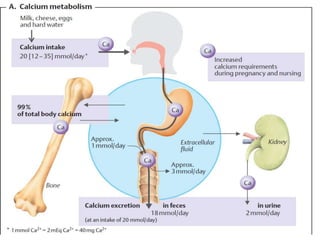
This document discusses calcium and phosphorus regulation in the body. It covers calcium and phosphorus metabolism, factors that regulate them, and their roles in tooth mineralization. Calcium is the most abundant mineral and is essential for skeletal structure, muscle function, nerve impulses, and other physiological processes. Homeostasis of calcium is maintained through dietary intake, absorption in the gut, and regulation by parathyroid hormone, calcitonin, vitamin D, and kidneys.




















































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)













