Downloaded 1,242 times


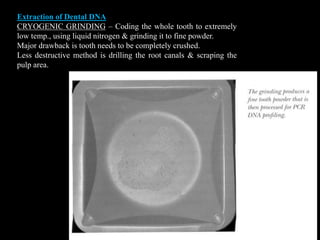
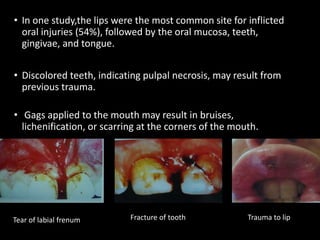
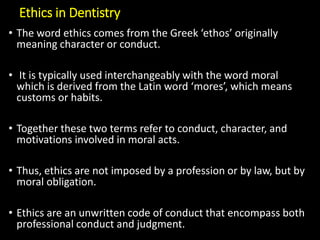
![Three Main forms of Dental Identification
1. Comparative identification
- most frequently performed examination
- to establish the remains of a decedent and a person
represented by ante mortem records are of the same
individual.
2. Reconstructive identification [Dental profiling or
Post-mortem Dental profile]
- elicit race, gender, age & occupation of the dead
individual
- undertaken when ante-mortem records are not
available.
3. Identification in mass disasters
- identification of victims in mass disasters](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-25-320.jpg)
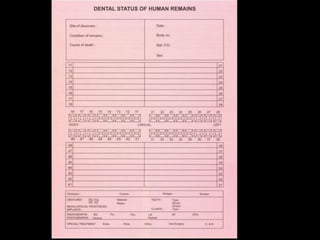
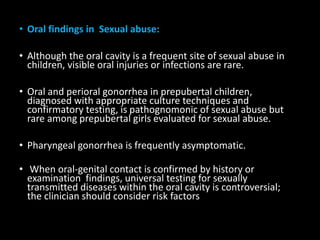
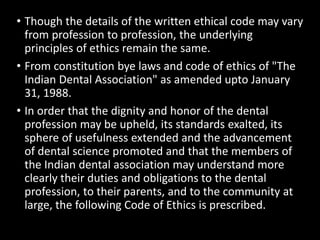
![A. ORAL AUTOPSY
– dissection to expose the organs, to determine the cause of death
– oral examination – essential part
– Forensic dentist should have knowledge about rigor mortis
[stiffening & rigidity], livor mortis [purple discoloration on the
skin in the dependent parts], decomposition & postmortem
artifacts
– For jaw separation, use of mouth gags or intra oral myotomy is
essential.
– Teeth to be reinforced with cyanoacrylate cement, polyvinyl
acetate or clear acrylic spray
– Thorough examination of soft tissue injuries, fractures &
foreign bodies
– information be entered on to the standard ‘Interpol Post-
Mortem form’ – Color coded in Pink.](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-27-320.jpg)

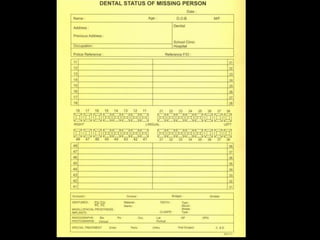
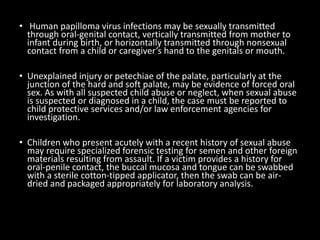
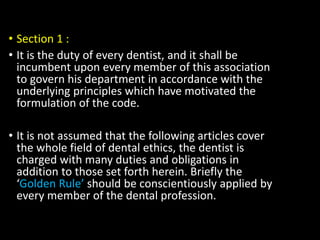
![B. OBTAINING DENTAL RECORDS
[Ante-mortem records]
– Contains information of treatment & dental status
during his/her life.
– Obtained from treating dentist, specialist or hospital
records – in the form of dental charts, radiographs, casts
& / or photographs
– Transcribed onto the standard ‘Interpol ante-mortem
form’ – color coded in Yellow.](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-30-320.jpg)
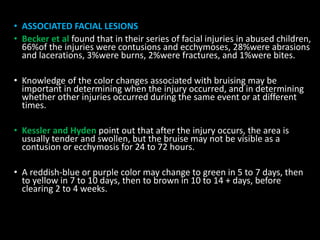
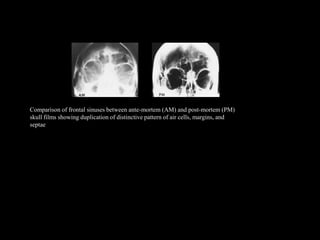
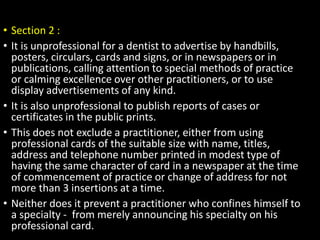
![C. COMPARING POST – AND ANTE-MORTEM
DENTAL RECORDS
– Compared by written notes, Study casts, radiographs,
Photographs etc.,
– Criteria for comparison are
a Tooth characteristics [number, eruption status,
position]
b. Personal characteristics
[crown morphology - occlusal ridges, cusps,
Root morphology - branching pattern, furcation,
fusion]
c. Complexity factors – tubercles, pits, additional
ridges, grooves, fissures &
d. Acquired features – hypoplasia, trauma, function,
personal habits, restorations](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-32-320.jpg)

![II. DENTAL PROFILING
[RECONSTRUCTIVE IDENTIFICATION (OR)
POST – MORTEM DENTAL PROILE]
It includes the decedent’s
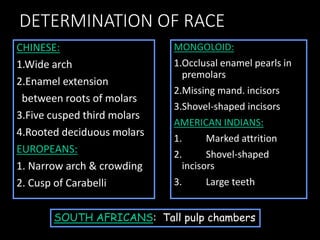
A. ETHNIC ORIGIN [Race determination]
B. GENDER [Sex determination]
C. AGE [Age estimation]](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-41-320.jpg)
![A. IDENTIFYING ETHNIC ORIGIN FROM TEETH
[RACE DETERMINATION]
Human species has been categorized into three races
– Caucasoid, Mongoloid & Negroid
Skull Face Nasal apertures
CAUCASIANS (White) Rounded Small Narrow & Elongated
MONGOLOIDS (Yellow) Square Large, Flattened Rounded
NEGROID
(Black Africans)
Narrow,
Elongated
Maxilla &
Mandible
Prognathic
Broad](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-42-320.jpg)

![IDENTIFICATION OF INDIVIDUAL’S ETHNIC
ORIGIN BASED PURELY ON DENTITION
Dental features - Combination of hereditary & environmental factors
Dental features are broadly categorized as
a) Metric [ Tooth size ] – Measurements
b) Non Metric [ Tooth Shape ]
- Presence or absence of a particular feature eg:- Cusp of carabelli
A. METRIC FEATURES:-
Influenced by local environmental factors eg:- missing lat.
Incisors causes compensatory increase in central incisors, Lack of
space result in compression of third molars.](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-45-320.jpg)
![2. SEX DIFFERENCES IN TOOTH SIZE
Generally teeth are smaller in females
Teeth – used for differentiating sex by measuring mesiodistal & buccolingual
dimensions
Canines – show max. sex difference
Mand. Canines show greatest dimensional difference, being larger in males
Dental Index
In addition to tooth size, tooth proportions have been suggested for differentiating
the sexes.
Aitchison presented the ‘Incisor Index’ [Ii] calculated by the formula
Ii = MDI2 MDI2 is the max. MD diameter of Max. LI
MDI1 MDI1 is the max. MD diameter of Max. CI
Ii is higher in males
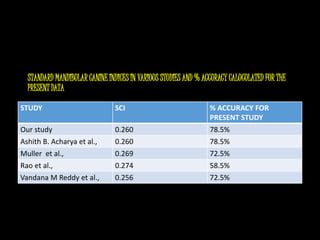
Standard Mandibular Canine Index Proposed by Rao & Assoc.
Mean mandibular canine index in female + S.D
+
Mean mandibular canine index in males – S.D
2
100](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-51-320.jpg)

![3. TOOTH MORPHOLOGY AND SEXING
According to scott & Turner II, ‘Distal Accessory ridge’ – a nonmetric
feature on the canine – most sexually dimorphic crown trait.
Males shows significantly higher frequency & more pronounced expression
than females.
4. SEX DETERMINATION BY DNA ANALYSIS
a. From pulp tissue:- Y chromosome analysis from dental pulp of male can be
done even after 1yr. Of death
b. From enamel protein [Amelogenin]:-
Amelogenin[AMEL] – Major matrix proteins secreted by the ameloblasts
of the enamel
AMELgene located on X & Y – chromosomes in humans
c. From Buccal Mucosa:- Barr bodies & x-chromosomes of female
detected from buccal mucosal epithelium.](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-55-320.jpg)
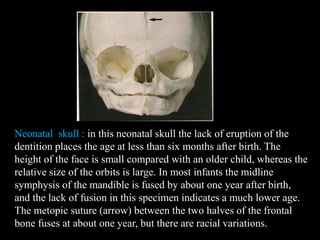
![SKELETAL AGE
DETERMINATION
Age Changes in Craniofacial Bones
Neonatal : Edentulous jaws, orbit size relatively
large
I year : Fusion of midline symphysis of
mandible
Metopic sutures of two halves of
frontal bone fuse
Lat. Sphenoidal synchondrose fuse
Fontanelles : Post & ant. Lateral fuse by 3 months.
Ant. Fontanelle by 1 ½ yr (18 MONTHS).
3 years : Condylar portion of occipital bone
fuses with squama
5 years : Condylar position of occipital bone
fuses with basoocciput.
SPHENOOCCIPITAL SYNCHONDROSIS
[between basal part of occipital bone & adj. body of
sphenoid] – Major skull cartilage centre, fuses by 18-
21 years – most useful skeletal ageing factor.](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-58-320.jpg)

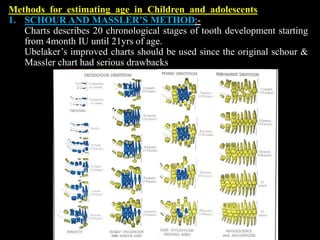
![B. AGE ESTIMATION IN CHILDREN AND ADOLESCENTS
1. Tooth emergence or Eruption
2. Tooth calcification
1. ERUPTION:- Convenient clinical method
visual assessment of teeth & compared with radiographs & charts.
Main drawback is emergence patterns are under the influence of
intraoral environment [infection, arch space, premature tooth loss]
2. CALCIFICATION:- better alternative, since,
a. Calcification can be observed for a period of several years from
radiographs
b. not altered by local factors
c. assess age at periods when no emergence takes place [2.5 – 6yrs
& more than 12yrs]](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-81-320.jpg)
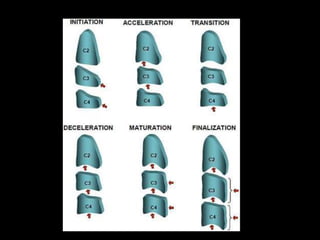
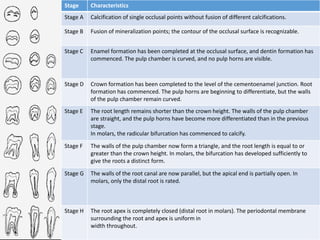
![2. DEMIRJIAN’S METHOD:-
- made up of scoring system
- development of seven mand.teeth was divided
into eight stages each [A to H].
- each tooth is assigned a maturity score that
corresponds to its developmental stage.
- maturity score for each tooth is added and a total
maturity score obtained
- Total maturity score is plotted on a chronologic
‘age conversion table’ [Separate for both sexes](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-83-320.jpg)
![Solheim suggested translucency length (in mm) or area
(mm2) measured on intact or sectioned teeth.
Two equations were given
Age = B0 + B1 + B2 X2 for zones of translucency ≤ 9mm
Age = B0 + B1 X for zones of translucency
>9mm
Where B0 is regression constant, B1 & B2 are regression
coefficients, X is the translucency length.
Disadvantages:-
1. Irregular junction of translucent & non translucent
zones.
2. Under estimation of age in old age groups due to
slowing down of dentinal sclerosis, restricting further ↑
in translucency
III) AGE ESTIMATION FROM INCREMENTAL
LINE OF CEMENTUM
Kagerer & Grupe suggested age estimation from
acellular cementum incremental lines.
Mineralized unstained cross-sections of teeth
[preferably mand. CI & 3rd molars] are used.](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-88-320.jpg)
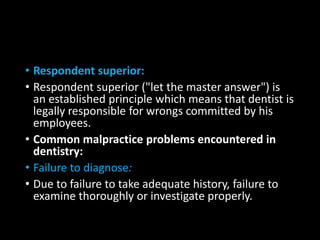
![THE PALATAL RUGAE IN IDENTIFICATION
[RUGOSCOPY]
Useful method in edentulous individuals
Rugae pattern – unique to an individual.
• The rugae pattern on the deceased's maxilla or maxillary
denture may be compared to old dentures that may be
recovered from the decedent's residence or plaster
models that may be available with the treating dentist.
• Palatal rugae are ridges on the anterior part of the palatal
mucosa on each side of the mid-palatine raphae, behind
the incisive papilla.
• These asymmetric and irregular ridges are well protected
by the lips, cheek, tongue, buccal pad of fat and teeth in
incidents of fire and high-impact trauma.](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-138-320.jpg)

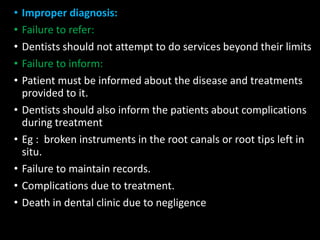
![• Cheiloscopy [Examination of lip prints]
• Cheiloscopy is a forensic investigation technique
that deals with identification of humans based on
lips traces.
• Lip prints have to be obtained within 24 hours of
time of death to prevent erroneous data that would
result from post mortem alterations of lip.
• Lip print pattern depends on whether mouth is
opened or closed.
• In closed mouth position lip exhibits well defined
grooves, where as in open position the groves are
relatively ill defined and difficult to interpret](https://image.slidesharecdn.com/rg6a7knmtimbztopivou-signature-a070450af8f7d3df13f45bce44fa322a737acadc7a7d2e5eedd3e1af3cf08b67-poli-150324125127-conversion-gate01/85/forensic-odontology-by-Dr-Revath-Vyas-Devulapalli-142-320.jpg)

This document provides an overview of forensic odontology, which involves the application of dental knowledge to legal investigations. It discusses the history of forensic dentistry dating back thousands of years, and defines key terms. The document is divided into sections covering personal identification through dental means, age and sex determination, and mass disaster management. Specific techniques used in odontology such as bite mark analysis and identification of race are explored. Comparative identification through dental records is explained in detail as the primary method of matching unknown remains to missing persons.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
