
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cementum ppt
Similar to Cementum ppt (20)
More from Dr. Mariyam Momin
More from Dr. Mariyam Momin (13)
Recently uploaded
Recently uploaded (20)
Cementum ppt
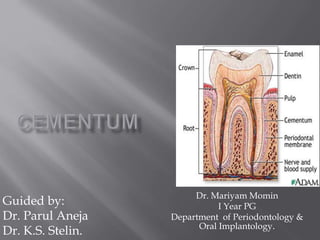
- 1. Dr. Mariyam Momin I Year PG Department of Periodontology & Oral Implantology. Guided by: Dr. Parul Aneja Dr. K.S. Stelin.
- 2. Introduction Definitions Physical characteristics Composition Cementogenesis Classification Acellular cementum Cellular cementum Cemental fibers Intermediate cementum Cemento-enamel junction (CEJ) Cemento-dentinal junction (CDJ) Functions Age changes in cementum Cemental resorption Cemental repair Abnormalities of cementum Influence of systemic disease on cementum Neoplasm associated cementum Clinical considerations Applied aspect Conclusion References
- 3. Cementum is the mineralized dental tissue covering the anatomic roots of human teeth. It was first demonstrated microscopically in 1835 by two pupils of Purkinje. It begins at the cervical portion of the tooth at the cemento-enamel junction and continues to the apex.
- 4. Cementum is a calcified avascular mesenchymal tissue that forms the outer covering of the anatomic root – Carranza. Cementum is a hard bone like tissue covering the anatomic roots of the teeth – Genco. Cementum is a calcified connective tissue which covers the root dentin and into which periodontal fiber bundles are inserted – Manson & Eley. Cementum is a hard bone like tissue covering the root surfaces and occasionally small portions of the crown of teeth – Lindhe. Cementum is a mineralized connective tissue that covers the roots of the teeth – Grant / Stern / Listgarten. Cementum is the mineralized dental tissue covering the anatomic roots of human teeth – Orbans.
- 5. Hardness: less than dentin. Color: light yellow in color and can be distinguished from enamel by its lack of luster and its darker hue. Cementum is somewhat lighter in color than dentin. The difference in color, however, is slight, and under clinical conditions it is not possible to distinguish cementum from dentin based on color alone. Permeability of cellular cementum is greater than that of acellular cementum. With age, the permeability of cementum decreases. Thinnest at CEJ (20-50 µm) Thickest towards the apex (150- 200µm).
- 6. Organic content and water – 50-55% Inorganic content - 45-50% Organic matrix of cementum consists of: Type I collagen (90%) Type III collagen (5%) Non collagenous proteins. BY VOLUME 45% inorganic 35% organic 20% water
- 7. Two main sources of collagen fibres 1. Sharpey’s fibers (Extrinsic) are the embedded portion of the principal fibers of periodontal ligament and formed by fibroblasts. 2. Fibers that belong to the cementum matrix (intrinsic) and produced by cementoblast. Due to its lower crystallanity of mineral component: - has the highest fluoride content - readily decalcifies in the presence of acidic conditions.
- 8. Non collagenous Non collagenous proteins play an important role in matrix deposition, initiation and control of mineralization and matrix remodelling. (Bone sialoprotein, osteopontin, tenascin, fibronectin, osteocalcin) Proteoglycans: Chondroitin sulphate, hyaluronate, heparan sulphate, biglycan and osteodherin. Growth factors: TGFᵝ, bone morphogenetic protein (BMP’s), platelet derived growth factor, osteoprotegerin. Cementum derived growth factor seen exclusively in cementum. - is an insulin like molecule. - Enhance proliferation of gingival fibroblasts and periodontal ligament cells.
- 9. Deposition of dentin along the inner aspect of HERS Breaking up of HERS allowing the newly formed dentin to come in contact with cells of dental follicle Differentiation of cementoblasts along the external surface of the root Protein secretion by cementoblasts mainly collagen & proteoglycans which forms the organic matrix of cementum Phase of matrix maturation, which subsequently mineralizes to form cementum.
- 11. Based on location 1. Radicular cementum 2. Coronal cementum Based on cellularity 1. Acellular cementum 2. Cellular cementum 3. Intermediate cementum
- 12. S.No. Cementum Origin Thickness Constituents 1 AAC Cementoblasts 1-15µm No cells & no fibers 2 AEFC Cementoblasts & fibroblasts 30-130µm Collagen fibers 3 CMSC Cementoblasts & fibroblasts 100-1000µm in apical 3rd Extrinsic & intrinsic fibers & cells 4 CIFC Cementoblasts Resorption lacunae Intrinsic fibers • Based on presence or absence of fibrils- Schroeder & Page 1. Acellular afibrillar cementum (AAC) 2. Acellular intrinsic fiber cementum (AIFC) 3. Acellular extrinsic fiber cementum (AEFC) 4. Cellular mixed stratified cementum (CMSC) 5. Cellular intrinsic fiber cementum (CIFC) 6. Intermediate cementum. Description of types of cementum
- 13. Acellular cementum It is the first formed cementum, hence it is known as primary cementum. It is called as acellular cementum, because it does not contain any cells. Cellular cementum It is also called as secondary cementum, forms after the tooth reaches occlusal plane. It is also called as cellular cementum because it contains cementocytes. Intermediate cementum 1. It is an ill-defined zone near the cemento-dentinal junctionof certain teeth that appears to contain cellular remnants of Hertwig’s epithelial root sheath embedded in a calcified ground substance. 2. It is an ill-defined zone extending from pre-CEJ to the apical1/3rd of the root. Acellular afibrillar cementum 1. It contains only the mineralized ground substance. It does not contain collagen fibers nor does it exhibit entrapped cementocytes. 2. It is a product of cementoblasts and is found almost exclusively on the enamel near the cemento-enamel junction with a thickness of 1-15µm.
- 14. Acellular intrinsic fiber cementum 1. It is the first formed cementum. 2. The collagen fibers are formed by cementoblasts & elaborated before the PDL formation. 3. The fibrous fringe of this cementum attaches to the PDL only after about 15-20µmof this cementum is formed. Acellular extrinsic fiber cementum 1. By definition it is composed primarily of Sharpey’s fibers of PDL but does not contain cementocytes. 2. Developmentally they come to occupy the coronal one half of the root surface. Its thickness is between 30-230µm. Cellular mixed stratified cementum It contains both intrinsic & extrinsic fibers &may contain cells.it is seen in apical third of the roots & furcation areas. Its thickness varies from 100-1000µm. Cellular intrinsic fiber cementum It contains only intrinsic fibers secreted by cementoblasts but not the extrinsic fibers.
- 15. Synonym – Primary cementum Acellular cementum is the first formed cementum, hence it is known as primary cementum. It is so called acellular cementum, as cells that form it (primary cementum) are not incorporated in it, but remain on its surface. Definition Cementum that forms in conjunction with root formation and tooth eruption is known as acellular cementum.
- 16. Composition Acellular cementum consists of fibers and calcified matrix. Calcified matrix - Ground substance Fibers 1. Sharpey’s fibers 2. Collagen fibers Structure 1. The cementum is thinnest at CEJ (10-15µm) & is thickest at the apex or bifurcation (150-200µm). 2. Acellular cementum is formed exclusively of intercellular substance; it is lamellated like bone and shows resting lines of period of inactivity.
- 17. Synonym – Secondary cementum Definition Cellular cementum is the cementum that forms after tooth eruption and in response to functional demand. Hence it is called as secondary cementum – Lindhe. Composition 1. Organic components – 50% 2. Inorganic components – 45-50% Thickness of cementum Area Thickness In coronal 3rd 16-60µm In apical 3rd 150-200µm In distal surface Thicker In mesial surface Thin
- 18. S.No. Features Acellular cementum Cellular cementum 1 Formation Forms before tooth reaches occlusal plane Forms after tooth reaches occlusal plane 2 Cells Does not contain any cells Contains cementocytes 3 Location Coronal portion of the root Apical portion of the root 4 Rate of formation Slower Faster 5 Incremental lines More Sparse 6 Function Forms after regenerative periodontal surgical procedure Contributes to the length of root during growth 7 Calcification More calcified Less calcified 8 Sharpey’s fibers More Less 9 Regularity Regular Irregular 10 Thickness Range from 30-50µm Thickness of 1 to several µm
- 19. Structure of cementum Cellular elements Formative cells 1. Cementoblasts 2. Cementocytes 3. Cementoids Degradative cells - Cementoclasts Matrix 1. Collagen fibers 2. Ground substance Other structural units 1. Incremental lines 2. Cemento-enamel junction (CEJ) 3. Cemento-dentinal junction (CDJ)
- 20. Cementoblasts Definition - Cementoblasts are the connective tissue cells, responsible for the formation of cementum. Structure 1. Cementoblasts develop from mesenchymal cells or fibroblasts, migrate through the proliferation of the root sheath and align themselves along the external border of dentin. 2. They may form a single or multi- cellular layer. They appear as cuboidal in single layer and fla in multi-layer. 3. These cells have centrally placed nucleus and the basophilic cytoplasm. Cytoplasm contains many mitochondria, golgi apparatus and RER. 4. Cementoblasts synthesize collagen and protein polysaccharides which make up organic matrix of cementum.
- 21. Cementocytes Synonym - Cement cells Definition - The trapped cementoblasts with the newly formed cellular cementum are called as cementocytes. Structure 1. The cells range from 8-15µm and may appear as round, oval or squamoid. 2. These cells have centrally placed nucleus and basophilic cytoplasm. 3. Cytoplasm contains mitochondria, golgi apparatus and endoplasmic reticulum. 4. Cementocytes are present in lacuna of cellular cementum and represents numerous protoplasmic cell processes. 5. Upto 30 cell processes may project from a single cell. Each process measures about 1µ in diameter and 15µm in length.
- 22. Orientation of cell processes 1. They may anastomose with each other. 2. In most cases processes are directed towards nutritional source. 3. Some processes are directed towards periodontal surface of cementum. 4. Some processes are directed towards periodontal surface and others towards dentin.
- 23. Cementoids Definition - Cementum immediately adjacent to PDL is not mineralized and is called as cementoid or pre- cementum. Structure 1. It begins at CEJ and proceeds to apical end. It is about 3-5 µm wideon the surface of acellular cementum and 1µm wide on the surface of cellular cementum. 2. Cementoid is predominantly composed by Sharpey’s fibers. In H-E stained section it is highly reflective and eosinophilic. 3. It forms outermost layer of cemental matrix and provides a protective environment for cementoblasts that resist cementum resorption.
- 24. Collagen fibers in cementum are of two types: External fibers External fibers are the Sharpey’s fibers of PDL, which are formed by the fibroblasts. Internal fibers 1. Internal fibers belong to the cementum, which forms the matrix of the cementum. 2. They are 1-2µmthick and are non-collagenous in the ordinary cementum.
- 25. Sharpey’s Fibers Definition - The terminal portion of the principle fibers that insert into the cementum and bone are termed as Sharpey’s fibers. Types 1. Severed fibers 2. Adhesive fibers Severed fibers - They are present within old bone and terminate at the reversal line which separates old bone from the new bone. Adhesive fibers - They cross the reversal line.
- 26. Origin & course 1. Sharpey’s fibers are the horizontal group of PDL fibers present immediately below alveolar crest fibers (or)apical to oblique fibers. They run in horizontal rows from cementum to alveolar processes. 2. They are mostly limited to coronal 3rd of PDL. They pass from their cemental attachment and cross PDL space and are inserted into alveolar processes as Sharpey’s fibers. Structure 1. Their size, number and distribution increases with function. 2. They are completely calcified with the mineral crystals oriented parallel to the fibrils, as they are in dentin and bone ,except in 10-50µm wide zone near the CEJ. Functions 1. Resist tipping forces. 2. Prevents lateral movement. 3. They make up most of the structure of the acellular cementum.
- 27. Incremental lines of Salter Due to continuous but phasic deposition of cementum, incremental lines can be seen in cementum, these are called as incremental lines of cementum / incremental lines of Salter.
- 28. Synonym – Layer of Hopewell Smith Definition Intermediate cementum is an ill-defined zone near cemento-dentinal junction of certain teeth that appear to contain cellular remnants of Hertwig’s sheath embedded in calcified ground substance – Carranza.
- 29. Features 1. It separates dentin from cementum which doesn’t have any features of dentin & cementum. 2. It is produced by alternations in phases of cementogenesis. It has been suggested that intermediate cementum is formed by epithelial cells of HERS. 3. It is an amorphous layer of non-collagenous material containing cementocytes or odontoblast processes. 4. It is predominantly seen in apical 2/3rd of roots of molars & premolars and is rarely observed in incisors. Functions 1. Seals the surface of sensitive root dentin. 2. It contains enamel like proteins, which help in the attachment of cementum to dentin.
- 30. The junction between enamel of crown and cementum of root of a tooth is called as CEJ. Fusion of cementum and enamel 1. (60-65%) – Cementum overlaps enamel 2. (30-35%) – Cementum meets enamel at butt joint 3. (10-5%) - Cementum separated from enamel. - In most cases cementum overlaps cervical enamel. This overlapping is caused by local degeneration of REE.
- 31. Clinical significance CEJ as a reference point 1. Junctional epithelial attachment is at the level of CEJ in healthy persons. 2. Rate of progression of periodontal disease can be studied from CEJ as areference point. Measurement of loss of attachment as CEJ is reference point - CEJ is used as the landmark for the assessment of loss of attachment. Other significances - If there is no union between the cementum and enamel, patient exhibits the hypersensitivity.
- 32. S.No. CEJ as reference Level of attachment 1 If the gingival margin is on anatomic crown then the loss of attachment is Pocket depth – distance from CEJ 2 If the gingival margin coincides with CEJ then the loss of attachment is Pocket depth 3 If the gingival margin is apical to CEJ then the loss of attachment is Pocket depth + distance from CEJ Clinical Significance
- 33. The terminal apical area of the cementum where it joins the internal root canal dentin is known as the cemento-dentinal junction. When root canal treatment is performed, the obturating material should be at the cemento-dentinal junction. There appears to be no increase or decrease in the width of the cemento- dentinal junction with age;its width appears to remain relatively stable. Scanning electron microscopy of the human teeth reveals that the cemento- dentinal junction is 2 to 3 μm wide. The fibril-poor layer contains asignificant amount of proteoglycans, and fibrils intermingle between the cementum and the dentin.
- 34. 1. It furnishes a medium for attachment of collagen fibers, which binds the tooth to the alveolar bone. 2. Its continuous deposition helps in achieving crown length lost due to attrition and maintains occlusal relationship. 3. It serves as a major reparative tissue for root surfaces, thereby maintaining integrity of the root surfaces. 4. It may also be viewed as the tissue that makes functional adaptation of teeth possible for eg; deposition of cementum in an apical area can compensate for loss of tooth substance from occlusal wear.
- 35. Cementum deposition appears to be continuous throughout life. Cementum deposition is less near CEJ and more in apical areas. Cemental deposition slows in old age.
- 36. Cementum undergoes resorptive changes. It may be alternative with periods of repair and deposition of new cementum.
- 37. Causes of cemental resorption Local factors 1. Cysts & tumors 2. Embedded teeth 3. Trauma from occlusion 4. Orthodontic tooth movement 5. Reimplanted and transplanted teeth 6. Teeth without functional antagonists 7. Periapical diseases or periodontal diseases. Systemic factors 1. Paget’s disease 2. Hypothyroidism 3. Calcium deficiency 4. Hereditary fibrous osteodystrophy. Types Based on location 1. Internal cemental resorption 2. External cemental resorption Based on the degree of persistence 1. Transient cemental resorption 2. Progressive cemental resorption
- 38. Appearance 1. Cementum resorption appears microscopically as bay like concavities in the root surface. Multi-nucleated giant cells & large mononuclear macrophages are generally found adjacent to cementum undergoing active resorption. 2. Cemental resorption is demarcated from root by a deeply staining irregular line called as reversal line. Reasons for relative resistance of cementum to resorption 1. Cementum is more resistant to resorption than is bone, and it is for this reason orthodontic tooth movement is made possible. 2. The difference in the resistance of bone and cementum to pressure my be caused by the fact that bone is richly vascularized whereas cementum is avascular, thus degenerative processes are much more easily effected by the interference with circulation in bone, whereas cementum with its slow metabolism (as in other avascular tissues) is not damaged by a pressure equal to that exerted on bone. 3. The surface layers of cementum contains more fluoride than does bone tissue, resulting in great resistance to the dissolution in acids produced by the osteoclast.
- 39. 1. After resorption has ceased the damage is repaired either by formation of acellular or cellular cementum or by alternate formation of both. 2. Newly formed cementum is demarcated from the root by deeply staining irregular line termed reversal line which delineates the border of previous resorption. Types of cemental repair 1. Anatomic repair 2. Functional repair Anatomic repair - In most cases of repair there is a tendency to reestablish the former outline of the root. This is called as anatomic repair. Functional repair - Where if only thin layer of cementum is deposited on the surface deep resorption, the root outline is not reconstructed and a bay like recess remains. - In such areas sometimes the PDL space is restored to its normal width by formation of bony projection so that proper functional relation is maintained . - This change is called as functional repair.
- 40. HYPERCEMENTOSIS Synonyms - Exostosis of root - Cementum hyperplasia Definition Hypercementosis refers to the prominent thickening of the cementum. It may be localized or generalized – Carranza. Causes Accelerated elongation of a tooth 1. It occurs due to lack of antagonist/ lack of tooth function. It occurs due to inherent tendency of the periodontium to maintain normal width of the PDL. 2. If cemental overgrowth is observed in roots of teeth for which antagonist of opposing arch is absent, it is called as dis-use hypertrophy. Inflammation of the root - It occurs at some distance above the apex as the inflammatory reaction acts as stimulation for the cementoblasts.
- 41. Tooth repair 1. Occlusal trauma results in mild root resorption and is then repaired by cementum formation. 2. Root fracture is also repaired on occasion by the deposition of cementum between the root fragments as well as in their periphery. Paget’s disease - It is a generalized skeletal disease characterized by excessive amount of cementum formation on roots of teeth (generalized) and by apparent disappearance of lamina dura of teeth. Other conditions 1. Hyperpituitarism 2. Cleidocranial dysostosis 3. Chronic inflammatory process 4. Chronic pulpal and periapical infections. Clinical features Age - It is predominantly seen in adults. Sites 1. Permanent teeth are affected more commonly than deciduous teeth. 2. Premolars are often affected and are often bilaterally affected & symmetrical in distribution.
- 42. Clinical presentation Signs - Teeth are vital and not sensitive to percussion. There may be difficulty in extraction. Symptoms - There is no increase or decrease in tooth sensitivity, unless periapical infection is present. Other features 1. In some cases hypercementosis is so extensive that it causes fusion of two or more teeth. 2. Roots appear large in diamete than normal and present as round apices. 3. There is formation of spikes on cementum, which can occur in cases of excessive occlusal trauma , probably due to deposition of irregular cementum in focal group of PDL fibers. Radiographic features 1. Lamina dura will follow the outline of teeth in normal PDL space. 2. There is thickening and apparent blunting of root with rounding of apex. 3. Apex appears as bulbous in some instances, after symmetric distribution of cementum. 4. There may be mildly irregular accumulation of cementum that is accommodated by related areas of bone resorption. Management - Treatment of primary cause.
- 43. Definition - A small portion of cementum forcibly separated either partially or completely, from the underlying dentin of the root as a result of occlusal force is known as cemental tear.
- 44. Causes 1. Acute trauma from occlusion can produce cemental tears with acute heavy traumatic forces. 2. The fragment of cementum could be detached by root planing or during periodontal sugery. Site of occurrence - The slip between the root and the fragment could occur along the cemento-dentinal border. Significance 1. The research result indicate that the cemental tear may be one of the contributing factors in the progression of adult periodontitis. 2. Cemental tear should be considered as a possible etiologic entity in localized rapid periodontal breakdown. 3. Cemental tear surfaces demonstrated a significantly greater loss of attachment than opposite intact surfaces. 4. Cemental tears if lying free in the periodontal ligament may resemble cementicles, particularly after they have undergone some remodeling through the resorption and subsequent repair.
- 45. Diagnosis - The diagnosis of cervical cemental tears can be made by characteristic feature which presents radiographically as a “prickle like body”. Management - Cemental tears are repaired by cementum growing into & filling the defects and eventually uniting with the torn cementum.
- 46. Fusion of cementum and alveolar bone with obliterated PDL. Occurs in teeth with cemental resorption After periodontal inflammation, tooth replantation, occlusal trauma. Results in resorption of root and its gradual replacement by bone. Lack physiological mobility, metallic percussion No proprioception because pressure receptors in periodontal ligament are deleted or not function correctly. Radiographically: Resorption lacunae are filled with bone. Periodontal ligament space is missing. Treatment: No predictable treatment can be suggested. Treatment modalities range from a conservative approach, such as restorative intervention to surgical extraction of affected tooth.
- 47. Abnormal, calcified bodies in the periodontal ligament. It has been postulated that they originate from foci of degenerating cells or epithelial rest cells. Generally less than 0.5mm in diameter. Types Free cementicles. Sessile or attached cementicles. Interstitial cementicles. As the cementum thickens with advancing age, it may envelop these bodies.
- 48. If some HERS cells remain attached to forming root surface, they can produce focal deposits of enamel like structures called enamel pearls.
- 49. Fusion of teeth by fusion of cementum, max. molars. Traumatic injury or crowding of teeth in the area during the apposition and maturation stage of development may be the cause. Difficulty in extraction
- 50. 1. HYPOPHOSPHATASIA Hypophosphatasia is a rare metabolic bone disease that is characterized by a deficiency of alkaline phosphatase. One of the first presenting signs of hypophosphatasia may be the premature loss of the primary teeth presumably caused by a lack of cementum on the root surfaces. The histopathologic examination of either a primary or permanent tooth that has been exfoliated from an affected patient often shows an absence or a marked reduction of cementum that covers the root's surface. Treatment: The treatment of hypophosphatasia is essentially symptomatic because the lack of alkaline phosphatase cannot be corrected
- 51. 2. PAGET’S DISEASE Paget’s disease is characterized by enhanced resorption of bone. Etiology: viral infection, inflammatory cause, autoimmune, connective tissue and vascular disorder. Clinical features Middle age and both males and females are affected. Involvement of facial bone. MAXILLA- progressive enlargement, alveolar ridge widened, palate flattened, tooth become loosened. MANDIBLE: findings are similar but not as severe as maxilla. Radiographic findings Cotton wool appearance of paget’s bone. Generalised hypercementosis of bone is seen Characteristic histologic feature Jigsaw or mosaic pattern. Treatment No specific treatment
- 52. 3. HYPERPITUITARISM Gigantism is the childhood version of growth hormone excess and is characterized by the general symmetrical overgrowth of the body parts. Prognathic mandible, frontal bossing, dental malocclusion, and interdental spacing are the other features. Intraoral radiograph may show hypercementosis of the roots. Acromegaly is characterized by an acquired progressive somatic disfigurement, mainly involving the face and extremities, but also many other organs, that are associated with systemic manifestations. Dental radiograph may demonstrate large pulp chambers and excessive deposition of cementum on the roots.
- 53. CEMENTOBLASTOMA The benign cementoblastoma is probably a true neoplasm of functional cementoblasts which form a large mass of cementum or cementum-like tissue on the tooth root. Clinical features Under age of 25 years. Mostly in mandible. (1st premolar) Slow growing, may cause expansion of cortical plates. Radiographic finding Radiographically, well circumscribed dense radio-opaque mass often surrounded by a thin, uniform radiolucent line. Treatment Extraction of tooth though pulp is vital as it might cause expansion of jaws
- 54. CEMENTIFYING FIBROMA The neoplasm is composed of fibrous tissue that contains a variable mixture of bony trabeculae, cementum like spherules or both. Origin of these tumors is odontogenic or from periodontal ligament. Clinical features 3rd and 4th decades of life. Female predilection. Mandibular premolar and molar are affected. Seldom cause any symptoms and are detected only on radiographic examination. Radiographic finding Radiographically, the lesion most often is well defined and unilocular it may appear completely radiolucent, or more often varying degrees of radiopacity. Treatment Enucleation of the tumor.
- 55. 1. Cementum is formed throughout life, this results in narrowing down of apical foramen. 2. With advanced age, the apical foramen may become narrowed down or even closed due to cementum deposition. Endodontic treatment of such teeth is difficult. 3. Cementum gives attachment to one end of PDL while the other end is held by alveolar bone. Due to forces of mastication, some PDL fibers get torn. These fibers are re-attached to cementum by fresh deposition of cementum. 4. Cementum is more resistant to resorption than bone. This is the basis for a judicious orthodontic movement. But excessive pressure during orthodontic treatment can cause resorption of cementum which can even extend over to dentin. 5. Cementoblastoma is a true neoplasm of cementum. Hypercementosis is a condition where excessive cementum formation takes place in response to infection. Role of cementum in periodontal diseases 1. Fusion of cementum and alveolar bone with obliteration of PDL is called ankylosis. It occurs in teeth with cemental resorption. 2. Exposure of cementum to oral environment occurs in cases gingival recession and as a consequence of loss of attachment in pocket formation. 3. Pathological processes can cause resorption of roots. Cementum becomes soft due to ineffective process and fails to give attachment to junctional epithelium.
- 56. Zander and Hurzeler(1958) stated that cementum is a better age estimating tissue than others. Incremental lines in cementum can be used as most reliable age marker than any other morphological or histological traits in skeleton. Evaluation of annual incremental lines of dental cementum is one of potentially valuable methods for biological age estimation in forensic anthropology and digitalized visual analysis system enhances the count and provides better results. (Bojarun et al,2003)
- 57. Cementum by its virtue of its structural dynamic qualities provide tooth attachment and maintains occlusal relationship. Fibers in cementum helps in tooth anchorage. Certain pathologic factors may cause irreversible damage to cementum else it is self reparartive to small disturbance.
- 58. Clinical Periodontology and Implant dentistry- Lindhe 4th Edition. Carranza’s Clinical Periodontology- 10th Edition. Orban’s oral histology and embryology- 12th Edition. TenCate’s Oral histology- 6th edition. PERIO 2000 - Dental cementum: the dynamic tissue covering of the root. Essentials of Periodontology – (Sahitya Reddy S)
Editor's Notes
- Description of types of cementum