
Downloaded 321 times






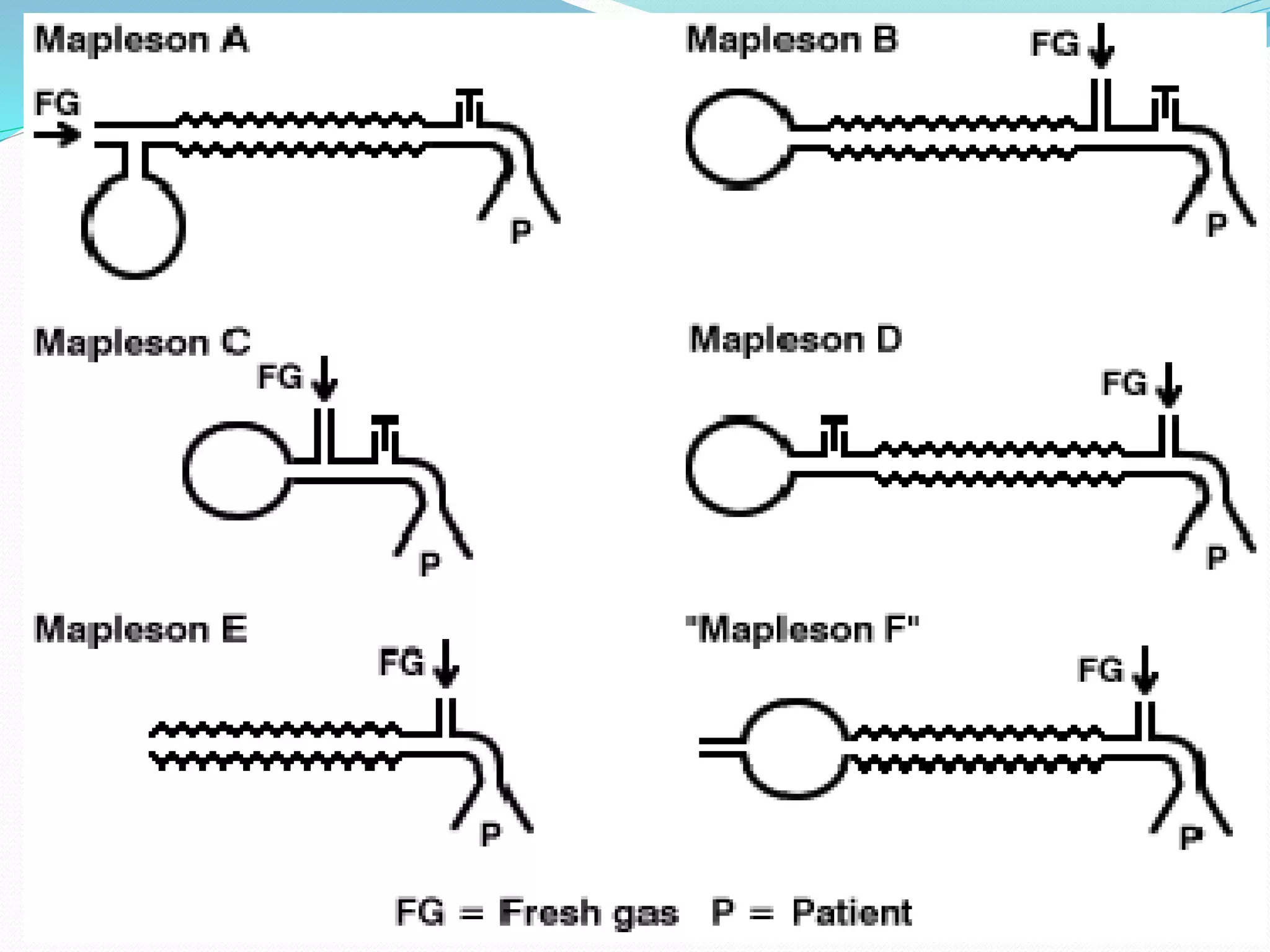

























This document discusses different types of breathing circuits used in anesthesia. It begins by introducing open, semi-closed, and closed breathing circuits. Open circuits are now obsolete and involved pouring anesthetic agents over a mask. Semi-closed circuits include Mapelson circuits A-F, with Type D (Bain) most commonly used for controlled ventilation. Closed circuits involve rebreathing of exhaled gases after carbon dioxide absorption by soda lime, making them very economical. Key components and properties of soda lime and factors affecting its carbon dioxide absorption are described.























































































