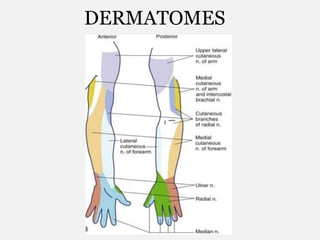
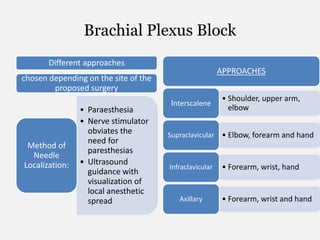
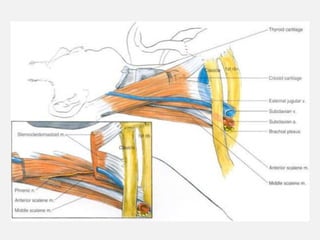
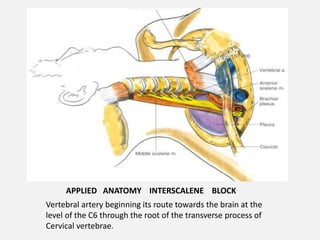
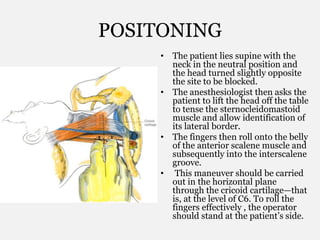
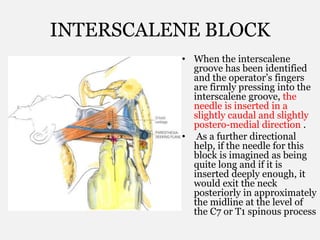
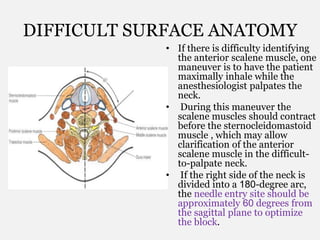
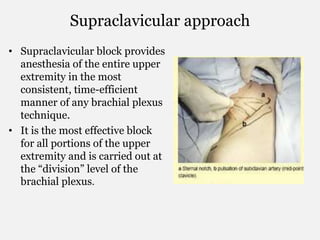
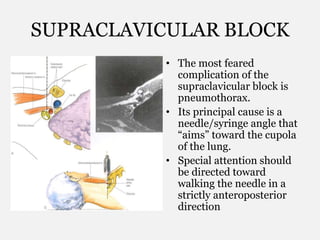
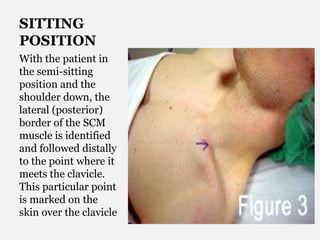
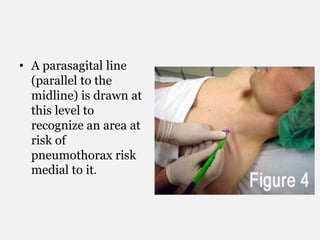
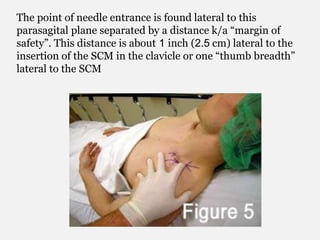
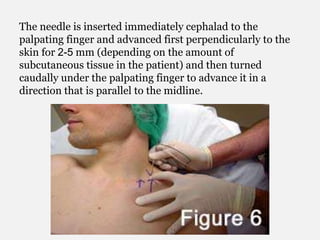
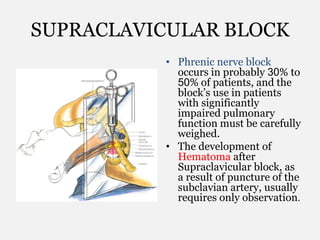
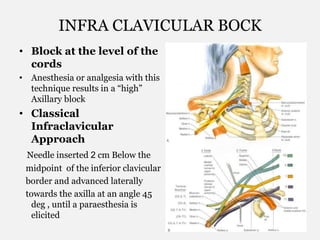
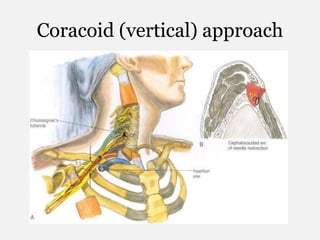
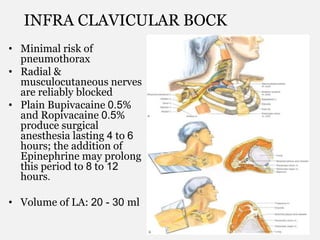
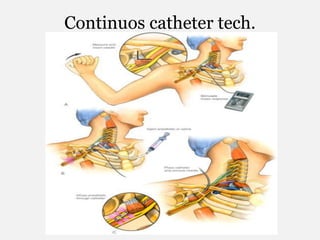
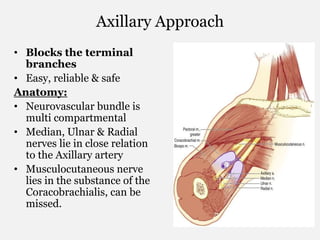
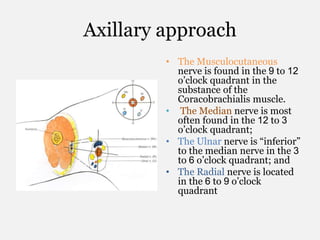
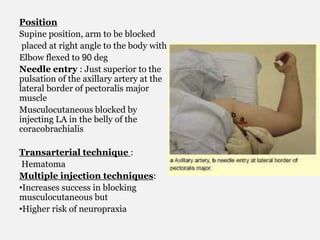
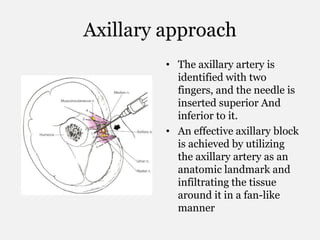
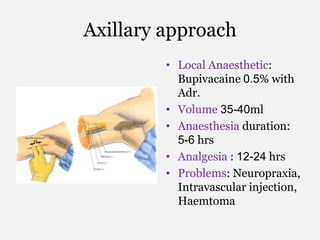
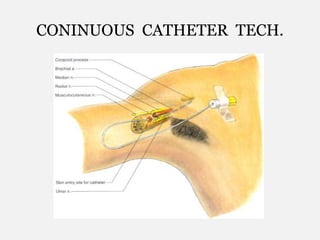
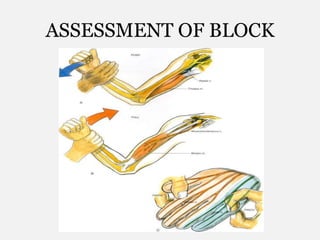
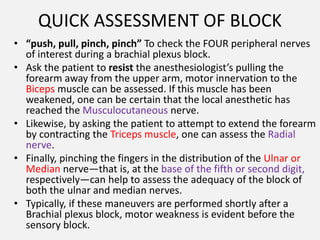
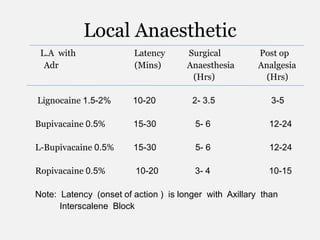
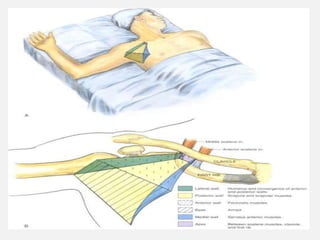
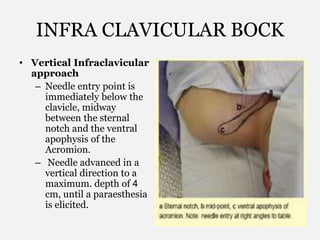
The document provides information about brachial plexus anatomy and different approaches for brachial plexus block, including interscalene, supraclavicular, infraclavicular, and axillary approaches. It discusses the anatomy relevant to each approach, positioning and needle placement techniques, methods for localizing nerves, injection procedures, expected durations and volumes of local anesthetic, and potential complications.