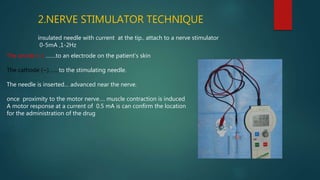
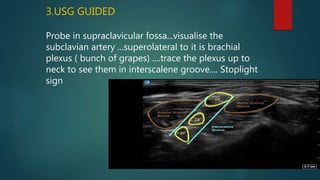
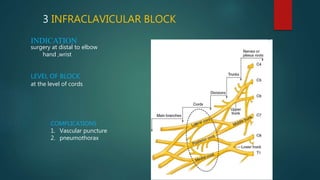
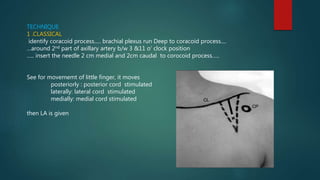
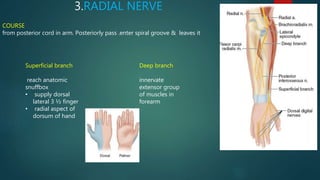
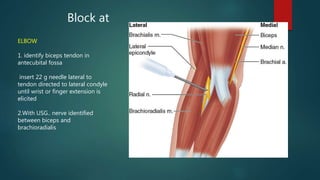
This document describes the anatomy and techniques for performing brachial plexus and upper limb nerve blocks. It begins with an overview of the brachial plexus formation from C5-T1 nerve roots and its branches. Various approaches for blocking portions of the plexus are then outlined, including interscalene, supraclavicular, infraclavicular, axillary blocks. Selective nerve blocks of the median, ulnar, radial and digital nerves are also reviewed. Clinical indications and contraindications are provided for each technique.