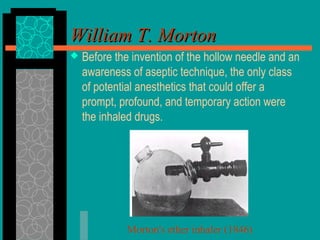
William Morton performed the first public demonstration of anesthesia on October 16, 1846, administering diethyl ether to patient Edward Abbott before neck surgery. Prior to this, various substances like alcohol, mandrake, and opioids soaked in sponges had been used throughout history in attempts to relieve surgical pain, but it was not until Morton's demonstration that inhalation of ether became widely accepted and practiced. This marked the beginning of modern anesthesia as a medical specialty. In subsequent decades, other inhaled anesthetic agents like nitrous oxide and chloroform were introduced and refined by pioneering anesthesiologists including John Snow, Joseph Clover, and Frederick Hewitt.
















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














