Downloaded 389 times
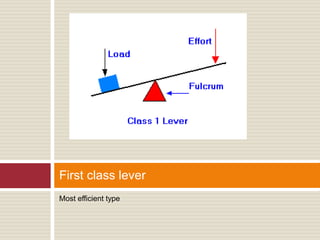
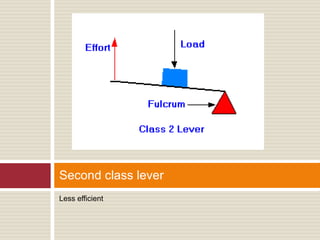
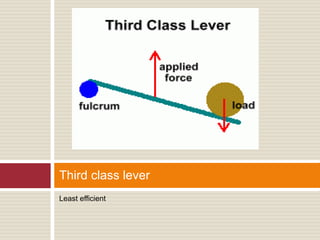
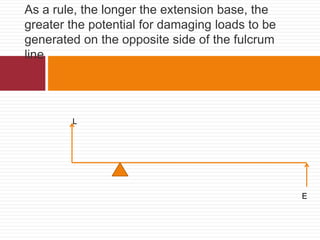


The document discusses biomechanical considerations in removable partial denture design. It notes that the primary goal is to control potentially damaging forces applied to the supporting structures, including bone and soft tissues. It describes the three classes of levers that a partial denture can act as when subjected to intraoral forces. Class I levers are most efficient while Class III are least efficient. Factors like extension base length can generate greater damaging loads. Removable partial dentures that are tooth-supported transmit forces axially like fixed bridges, while tissue-supported designs can result in non-axial loading and greater potential for damage over time. Control of forces is important through factors like tissue health and component positioning.































































































