Downloaded 148 times



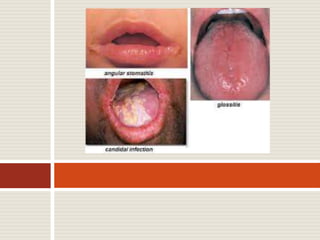
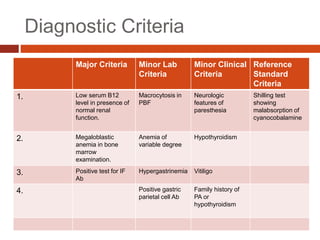

Vitamin B12 deficiency, also known as pernicious anemia, is an autoimmune disorder where antibodies block intrinsic factor and prevent vitamin B12 absorption from the stomach, leading to megaloblastic anemia. It presents with weakness, sore tongue, and neurological or gastrointestinal issues. Laboratory findings include macrocytic anemia, elevated MCV, hypersegmented neutrophils, and low serum B12 levels. The gold standard test is gastric biopsy showing parietal cell atrophy. Treatment is lifelong vitamin B12 supplementation by injection or oral administration.











































































