Definition
• Haemostasis isderived from a Greek word, which
means stoppage of blood
• A physiological process that helps to maintain blood in
the fluid state, prevent the escape of blood from
damaged vessel through clot formation and
dissolution of clot after healing
• The aims of the normal haemostatic process are to
prevent blood loss from intact vessels and to arrest
bleeding from injured vessels
3.
08/23/2025 3
INTRODUCTION
• Haemostasisis a complex physiologic processes that :
keeps blood in a fluid state
Ensures blood clot formation so as to arrest a bleed,
Confines clot to the site of injury
That ensures clot dissolution as part of healing process.
4.
Introduction
• Haemostasis refersto the process whereby blood coagulation is
initiated and terminated in a tightly regulated fashion, together with
the removal (or fibrinolysis) of the clot as part of vascular remodeling;
as such, haemostasis describes the global process by which vessel
integrity and patency are maintained over the whole organism, for its
lifetime.
5.
Overview of Haemostasis
•The subsystems of haemostasis are not independent
• The whole mechanism is integrated in vivo
• The thrombin generated is localized and limited to the site of injury
• The accompanying fibrinolysis and tissue remodeling is also localized
• Thrombin generation is not a simple exponential cascade
• It is a complex network of interactions with positive and negative
feedback loops
6.
What initiates bloodcoagulation ?
• Exposure of blood to cells expressing tissue factor on their surfaces is
necessary and sufficient to initiate blood coagulation in vivo
• Tissue factor is expressed at biological boundaries such as skin, organ
surfaces, vascular adventitia etc.
7.
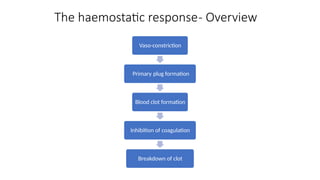
The haemostatic response-Overview
Vaso-constriction
Primary plug formation
Blood clot formation
Inhibition of coagulation
Breakdown of clot
8.
Role of bloodvessels
• Immediate vasoconstriction of the injured vessel (due to vascular
smooth muscle cells)
• Reflex constriction of adjacent small arteries and arterioles is
responsible for an initial slowing of blood flow to the area of injury.
• The reduced blood flow allows contact activation of platelets and
coagulation factors.
9.
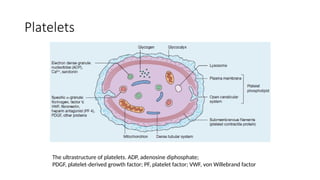
Platelets
The ultrastructure ofplatelets. ADP, adenosine diphosphate;
PDGF, platelet derived growth factor; PF, platelet factor; VWF, von Willebrand factor
‐
10.
Platelets
• Platelets areinvolved in the formation of mechanical
plug during the haemostatic response to vascular
injury
• They also provide procoagulant surface for the
reactions of the coagulation system.
11.
Role of Platelets
•Platelets bind to damaged endothelium or sub-endothelium to form a
primary haemostatic plug, platelet plug to prevent or limit blood loss.
• Activities include:
- adhesion
- aggregation
- release
- contraction
13.
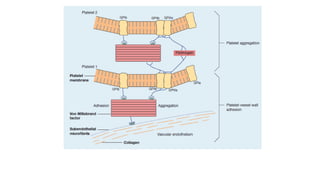
Platelet function- Adhesion
•Adhere to sub-endothelium at the site of injury
• Coating of the subendothelial collagen by vWF accelerates adhesion
by a receptor-mediated process….. Platelet GPIb binds to vWF on the
damaged surface.
14.
Platelet function- Aggregation
•Platelet sticks to each other to build an adequate platelet mass for
primary haemostasis.
• Conformational change induces expression of GPIIb-IIIa. This further
enhances aggregation by binding to vWF.
• Platelets release preformed granules, alpha and dense granules.
15.
Platelet function- Shapechange
• Upon activation, platelets become spherical and extend pseudopodia
to enable them to attach to other platelets and to the vessel wall.
• Shape change is mediated by phosphorylation of myosin light chains,
as a consequence of elevation of intracellular Calcium ions which
activate myosin light chain kinase.
16.
COAGULATION CASCADE
• Ahighly regulated cascade of reactions that form a variety of products
involved in haemostasis.
• Participants include:
1. Enzymatic coagulation factors: II, VII, IX, X, XI, XII, XIII, prekallikrein
2. Non-enzymatic cofactors: I, III, V, VIII, High Molecular Weight
Kininogen, Ca, phospholipids.
17.
Blood coagulation
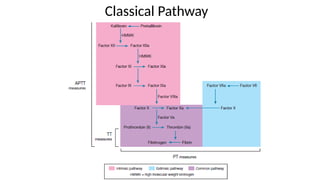
Coagulation Cascade
•It has been traditionally classified into intrinsic and
extrinsic pathways, both of which converge on factor
X activation.
• The classical theory of blood coagulation is
particularly useful for understanding the in vitro
coagulation tests.
• Fails to incorporate the central role of cell-based
surfaces in in vivo coagulation process
Cell based theory-Coagulation in vivo
• Thrombin generation is dependent on three enzyme
complexes
• Each consisting of protease, cofactor, phospholipids
(PL) and calcium.
• Extrinsic Xase (VIIa, TF, PL, Ca2+) generating FXa;
• Intrinsic Xase (IXa, VIIIa, PL, Ca2+) also generating FXa;
• Prothrombinase complex (Xa, Va, PL, Ca2+) generating
thrombin.
20.
Natural Inhibitors ofCoagulation
• Tissue factor pathway inhibitor (tFPI)
• Inhibits tissue factor, Xa, VIIa
• Antithrombin
• Inactivates thrombin
• Heparin Cofactor II
• Inhibits thrombin
• Proteins C and S
21.
Fibrinolytic pathway
• Fibrinolyticsystem functions to remove fibrin from
intravascular and extravascular sites to prevent
thrombosis and haemorrhage.
• The components include
• The proenzyme; plasminogen
• Plasminogen activators
• Fibrinolytic inhibitors
• One group is made up of inhibitors of plasminogen activators e.g.
t-PA inhibitors (PAI-1, PAI-2), alpha l anti-trypsin, C1 esterase
inhibitor, alpha2 antiplasmin and alpha2 macroglobulin.
• A second group consists of inhibitors of plasmin
22.
Tests of haemostaticfunction
• Platelet count & blood film examination
• Screening test for coagulation
• Prothrombin time (PT)
• Activated Thromboplastin time (APTT)
• Thrombin time (TT)
• Specific assays of coagulation factors
• Tests of platelet function
• Platelet aggregometry
• Test of fibrinolysis
23.
Tests of haemostaticfunction
Prothrombin time (PT)
• The prothrombin time (PT) measures factors VII, X, V,
prothrombin and fibrinogen.
• Tissue thromboplastin (a brain extract) or [synthetic]
tissue factor with lipids and calcium is added to
citrated plasma.
• The normal time for clotting is 10–14 s.
• It is often expressed as the international normalized
ratio (INR)
24.
Tests of haemostaticfunction
Activated Thromboplastin time (APTT)
• APTT measures factors VIII, IX, XI and XII in addition
to factors X, V, prothrombin and fibrinogen.
• Three substances – phospholipid, a surface activator
(e.g. kaolin) and calcium – are added to citrated
plasma.
• Normal time for clotting is approximately 30–40 s.
25.
Tests of haemostaticfunction
Thrombin Time (TT)
• It is sensitive to a deficiency of fibrinogen or inhibition
of thrombin.
• Diluted bovine thrombin is added to citrated plasma
at a concentration giving a clotting time of 14–16 s
with normal subjects
• Patient’s TT should be within 2s of the control
26.
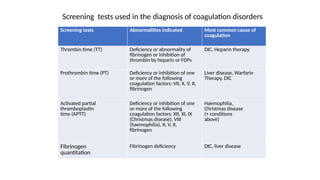
Screening tests Abnormalitiesindicated Most common cause of
coagulation
Thrombin time (TT) Deficiency or abnormality of
fibrinogen or inhibition of
thrombin by heparin or FDPs
DIC, Heparin therapy
Prothrombin time (PT) Deficiency or inhibition of one
or more of the following
coagulation factors: VII, X, V, II,
fibrinogen
Liver disease, Warfarin
Therapy, DIC
Activated partial
thromboplastin
time (APTT)
Deficiency or inhibition of one
or more of the following
coagulation factors: XII, XI, IX
(Christmas disease), VIII
(haemophilia), X, V, II,
fibrinogen
Haemophilia,
Christmas disease
(+ conditions
above)
Fibrinogen
quantitation
Fibrinogen deficiency DIC, liver disease
Screening tests used in the diagnosis of coagulation disorders
27.
Conclusion
• Haemostasis isa complex physiological process for
maintaining the fluidity of blood.
• It is regulated by delicate balance existing between
thrombogenic and anti thrombogenic mechanisms
present in the body.
• Normal haemostasis requires vasoconstriction, platelet
aggregation, blood coagulation and fibrinolysis
• Imbalance in haemostatic mechanisms will predispose an
individual to either bleed or present with thrombosis.

![Tests of haemostatic function
Prothrombin time (PT)
• The prothrombin time (PT) measures factors VII, X, V,
prothrombin and fibrinogen.
• Tissue thromboplastin (a brain extract) or [synthetic]
tissue factor with lipids and calcium is added to
citrated plasma.
• The normal time for clotting is 10–14 s.
• It is often expressed as the international normalized
ratio (INR)](https://image.slidesharecdn.com/5-250823143147-5b804947/85/5-Normal-Haemostasis_MS-PPTX-presentation-23-320.jpg)