
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Blepharitis
Similar to Blepharitis (20)
More from Priya
More from Priya (20)
Recently uploaded
Recently uploaded (20)
Blepharitis
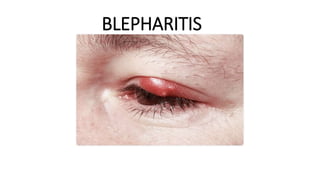
- 1. BLEPHARITIS
- 2. INTRODUCTION Blepharitis is one of the most common ocular disorders encountered in clinical practice. In a survey of US ophthalmologists and optometrists, 37% to 47% of patients seen by those surveyed had signs of blepharitis. Apart from some regional studies, however, few epidemiologic data exist that estimate its true prevalence in the general population. A recent cross-sectional study in Spain based on a randomly selected sample population reported rates of asymptomatic and symptomatic meibomian gland dysfunction of 21.9% and 8.6% of individuals, respectively. Blepharitis can affect all age and ethnic groups. One single-center study of 90 patients with chronic blepharitis found that the mean age of patients was 50 years. Compared with patients with other forms of blepharitis, patients with staphylococcal blepharitis were found to be relatively younger (42 years old) and mostly female (80%).[
- 3. DEFINTION Blepharitis, an inflammatory condition of the eyelid margin
- 4. TYPES Blepharitis is classified into three types: •Anterior blepharitis •Posterior blepharitis •Mixed blepharitis In anterior blepharitis, the eyelid skin, base, and follicles of the eyelashes are affected—the outside of the eyelid, in the front edge attached to the eyelashes. Posterior blepharitis occurs at the inner edge, the eyelid that is in contact with the eyeball. In some patients, both anterior and posterior type of blepharitis can occur, which is termed as mixed blepharitis.
- 5. CAUSES Anterior Blepharitis Staphylococcal infections or seborrheic dermatitis is the main cause of anterior blepharitis. Staphylococcal infections Although Staphylococcus bacteria are commonly present in the skin, nose, buttocks, and the surface of the armpits, they can enter the human body through a cut or insect bite in the skin or through skin openings while using medical equipment (for example, urinary catheters). Seborrhoeic Dermatitis Seborrhoeic dermatitis is a type of eczema visible in places where the sebaceous glands are active. Sebum production is, however, not related to the severity of the eczema. Some individuals are free from eczema even though the sebum production is higher. Though the exact cause of Seborrhoeic dermatitis is not understood completely, conditions such as depression, epilepsy, heavy intake of alcohol, and medications such as psoralen, lithium, and interferon induce the risk of Seborrhoeic dermatitis.
- 6. Causes of Posterior Blepharitis In posterior blepharitis, problems are associated with the inner part of the eyelid. The eyelid margins have minute oil glands, called meibomian glands. These are positioned in both the lower and upper eyelids with each lid carrying 15–20 glands. The openings of the glands lie inside the line of the eyelash, typically on the eyelid edges. The oil percolates slowly when the eyes are blinked; however, the gland collapses when it is empty. The oil produced by this gland merges with the watery component in the eye and together a tear film is created. This oily layer provides a coating to the water layer and protects the water from evaporation. When the quality or quantity of the water or oil is altered, there are symptoms such as eye irritation.
- 7. RISK FACTORS •Seborrheic dermatitis Seborrheic dermatitis, characterized by flaking and greasy skin on the scalp, retro auricular area, glabella, and nasolabial folds, has been reported in 33% to 46% of patients with blepharitis. In one study, 95% of patients with seborrheic blepharitis also had seborrheic dermatitis •Acne rosaceaAcne rosacea has been reported in 20% to 42% of patients with all types of blepharitis Characteristic facial skin findings include erythema, telangiectasias, papules, pustules, and prominent sebaceous glands. •Contact allergies •Chemical irritants •Poor hygiene •Cosmetic makeup •Advanced age •Diabetes .Dry Eyehas been reported to be present in 50% of patients with staphylococcal blepharitis.Conversely, in a series of 66 patients with dry eye, 75% were reported to have staphylococcal conjunctivitis or blepharitis
- 9. SIGNS AND SYMPTOMS •Watery eyes •Red eyes •A gritty, burning or stinging sensation in the eyes •Eyelids that appear greasy •Itchy eyelids •Red, swollen eyelids •Flaking of the skin around the eyes •Crusted eyelashes •Eyelid sticking •More frequent blinking •Sensitivity to light •Blurred vision that usually improves with blinking
- 10. DIAGNOSTIC EVALUATION A Schirmer's test can measure the amount of moisture bathing the eye. This test is useful for determining the severity of the condition. A five-minute Schirmer's test with and without anesthesia using a Whatman #41 filter paper 5 mm wide by 35 mm long is performed. For this test, wetting under 5 mm with or If the results for the Schirmer's test are abnormal, a Schirmer II test can be performed to measure reflex secretion. In this test, the nasal mucosa is irritated with a cotton-tipped applicator, after which tear production is measured with a Whatman #41 filter paper. For this test, wetting under 15 mm after five minutes is considered abnormal without anesthesia is considered diagnostic for dry eyes. Tear break-up time (TBUT) also known as tear film break-up time (TFBUT) is the time taken to appear first dry spot on cornea after a complete blinking . TFBUT measurement is an easy and fast method used to assess the stability of tear film. It is a standard diagnostic procedure in the dry eye clinics. The volume of tear in the eye depends on two factors, drainage through the lacrimal passages and evaporation. Culture and sensitivity to find out the causative organism
- 11. MANAGEMENT•Routine cleaning of eyelids once or twice a day and keep it without crust. •Apply warm compresses on the eyelid that can loosen the crust, bacteria, dust, and grime, and reduce inflammation. •Push out excessive oil accumulated in the gland by lightly massaging the eyelids. •Dilute some baby shampoo in warm water and apply it on the eyelids. Gently scour the eyelids using a cotton swab for about 15 sec or soak a cotton ball in the shampoo mixture and cautiously apply it on the eyelashes. Finally, wash the eyelids and eyelashes using warm water. •When dandruff is present in the scalp, it is recommended to use anti-dandruff shampoo or anti- bacterial shampoo to wash the hair and scalp Topical ointments such as bacitracin or erythromycin may be applied to the eyelid margins one or more times daily or before bed for two to eight weeks or until symptoms resolve. Some patients require chronic therapy in order to remain symptom free.[Oral antibiotics such as tetracyclines (tetracycline, doxycycline, minocycline) or macrolides (erythromycin, azithromycin) are recommended for patients with MGD not controlled with eyelid hygiene or patients with associated rosacea. Corticosteroid drops or ointment can be applied several times daily to the eyelids or ocular surface until the inflammation is reduced. Topical lubricant should be applied eg hypo tears,tears again,oasis tears.
- 12. Increased intake of essential fatty acids, specifically omega-3 fatty acid, was recommended by the International Workshop on MGD for cases of mild-to- severe MGD. These essential fatty acids may be beneficial to anti- inflammatory processes and have also been associated with reduced dry eye symptoms. For patients with Demodex infestation who have failed conventional treatment methods, 50% tea-tree oil eyelid scrubs and daily tea-tree-oil shampoo scrubs have been shown to be of some benefit when used for a minimum of 6 weeks. Oral ivermectin has also been reported to be useful in some cases of recalcitrant Demodex blepharitis thermal pulsation system that applies heat and pressure to the eyelid tissue simultaneously to express the meibomian glands .A small, prospective study found that a single 12-minute treatment with the Lipiflow system gave rise to significant improvement in both signs Intraductal meibomian gland probing to reopen MG orfices mechanically has been reported to provide rapid and lasting symptom relief in a case series of patients with obstructive MGD, but can be uncomfortable and inconvenient for patients
- 13. COMPLICATION •Eyelash problems. Blepharitis can cause your eyelashes to fall out, grow abnormally (misdirected eyelashes) or lose color. •Eyelid skin problems. Scarring can develop on your eyelids from long-term blepharitis. Or the eyelid edges might turn inward or outward. •Excess tearing or dry eyes. Abnormal oily secretions and other debris shed from the eyelids, such as flaking associated with dandruff, can build up in your tear film — the water, oil and mucus solution that forms tears. •Abnormal tear film interferes with keeping your eyelids moist. This can irritate your eyes and cause symptoms of dry eyes or excess tearing. •Sty. A sty is an infection that develops near the base of the eyelashes. The result is a painful lump on the edge of your eyelid. A sty is usually most visible on the surface of the eyelid. •Chalazion. A chalazion occurs when there's a blockage in one of the small oil glands at the margin of the eyelid, just behind the eyelashes. This blockage causes inflammation of the gland, which makes the eyelid swell and redden. This can clear up or turn into a hard, nontender bump. •Chronic pink eye. Blepharitis can lead to recurrent bouts of pink eye (conjunctivitis). •Injury to the cornea. Constant irritation from inflamed eyelids or misdirected eyelashes can cause a sore to develop on your cornea. Not having enough tears could increase your risk of a corneal infection.
- 14. PREVENTION 1.Keep hands and face clean. 2.Resist the urge to touch itchy eyes/face. Use a clean tissue if you must. 3.Remove all eye makeup before bedtime. 4.Wipe away excess tears or eye drops with a clean tissue. 5.Wear glasses instead of contact lenses until the condition clears