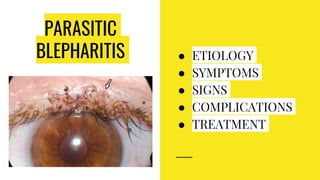
Blepharitis is a chronic inflammation of the eyelid margins with various types including bacterial, seborrheic, and meibomitis, each having distinct symptoms and treatments. Symptoms may include irritation, itching, and the presence of crusts, while treatments range from hygiene practices to antibiotics and steroid eye drops. Complications can include madarosis, styes, and dry eyes if not properly managed.




















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















