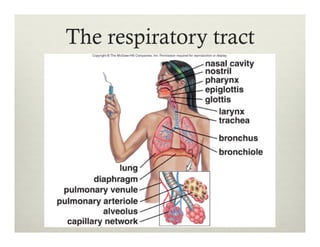
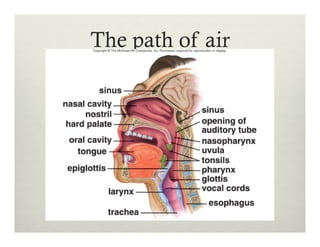
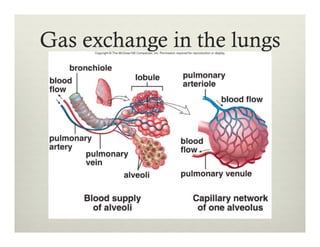
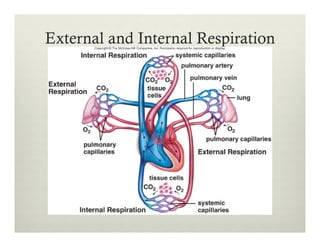
The respiratory system allows for gas exchange through breathing. Air enters the nose and travels through the pharynx, larynx, trachea, bronchi and bronchioles to the alveoli in the lungs. In the alveoli, oxygen diffuses into the bloodstream and carbon dioxide diffuses out. The blood carries oxygen to tissues and removes carbon dioxide through external and internal respiration.