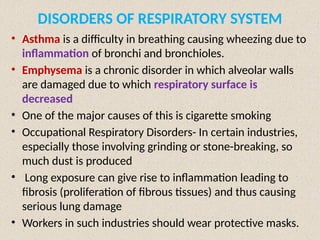
The document details the respiratory systems across various organisms, highlighting the mechanisms of gas exchange through diffusion, gills, and lungs. It describes the human respiratory system components including the conducting and exchange parts, mechanisms of breathing, and respiratory volumes and capacities. The processes of oxygen and carbon dioxide transport and the regulation of respiration are explained, along with common respiratory disorders like asthma and emphysema.







![breathing and exchange of gases (1).pptx [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/breathingandexchangeofgases1-250919170828-d5147614-thumbnail.jpg?width=640&height=640&fit=bounds)













































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
