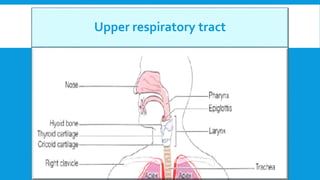
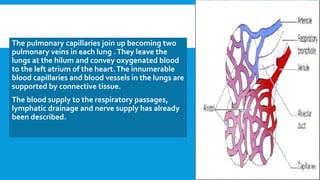
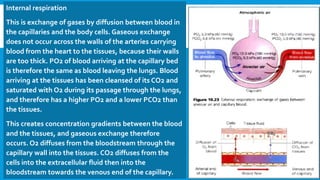
The document discusses the anatomy and functions of the respiratory system, detailing the roles of the upper and lower respiratory tracts in air passage, gas exchange, and respiratory mechanics. It explains the processes involved in inhalation and exhalation, as well as the exchange of oxygen and carbon dioxide in the alveoli and tissues. Additionally, it covers the regulation of respiration by the nervous system and the influence of various factors on breathing patterns.

![Chemoreceptors
These are receptors that respond to changes in the partial pressures of oxygen and carbon
dioxide in the blood and cerebrospinal fluid.They are located centrally and peripherally.
Central chemoreceptors.These are on the surface of the medulla oblongata and are bathed
in cerebrospinal fluid. When the arterial PCO2 rises (hypercapnia), even slightly, the central
chemoreceptors respond by stimulating the respiratory center, increasing ventilation of
the lungs and reducing arterial PCO2.The sensitivity of the central chemoreceptors to
raised arterial PCO2 is the most important factor in maintaining homeostasis of blood
gases in health. A small reduction in PO2 (hypoxaemia) has the same, but less pronounced
effect, but a substantial reduction has a depressing effect.
Peripheral chemoreceptors. These are situated in the arch of the aorta and in the carotid
bodies.They are more sensitive to small rises in arterial PCO2 than to similarly low arterial
PO2 levels. Nerve impulses, generated in the peripheral chemoreceptors, are conveyed by
the glossopharyngeal and vagus nerves to the medulla and stimulate the respiratory
center.The rate and depth of breathing are then increased. An increase in blood acidity
(decreased pH or raised [H+]) stimulates the peripheral chemoreceptors, resulting in
increased ventilation, increased CO2 excretion and increased blood pH.](https://image.slidesharecdn.com/4respiratorysystem-230612073909-b8755d88/85/Respiratory-system-ppsx-19-320.jpg)



![Respiratory system final [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/respiratorysystemfinalautosavedautosaved-250830120123-8e8c0dcb-thumbnail.jpg?width=640&height=640&fit=bounds)