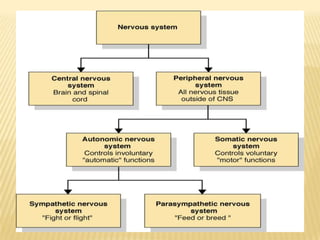
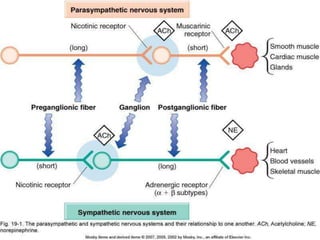
The document discusses drugs that act on the autonomic nervous system, including:
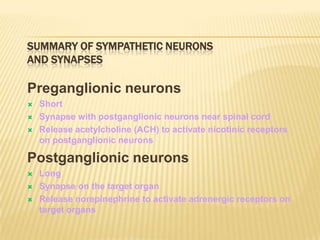
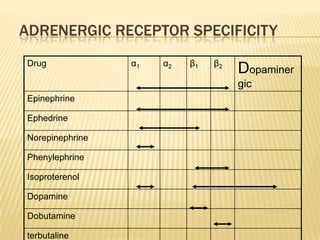
- Adrenergic drugs that stimulate the sympathetic nervous system by mimicking norepinephrine and epinephrine. This includes both catecholamines and non-catecholamines.
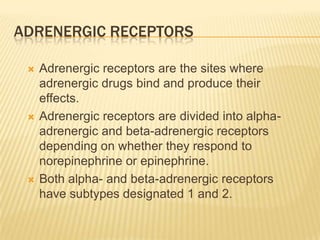
- Adrenergic blockers that block the actions of norepinephrine and epinephrine at adrenergic receptor sites. This includes both alpha-blockers and beta-blockers.
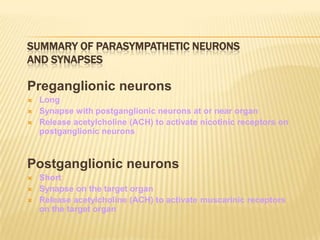
- Cholinergic drugs that stimulate the parasympathetic nervous system by mimicking acetylcholine, and anticholinergic drugs that block acetylcholine's actions. Cholinergic drugs can be direct-acting or indirect-























































![drugs that affect the autonomic nervous system.ppt [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/finaldrugsthataffecttheautonomicnervoussystem-181221100012-thumbnail.jpg?width=640&height=640&fit=bounds)



















































