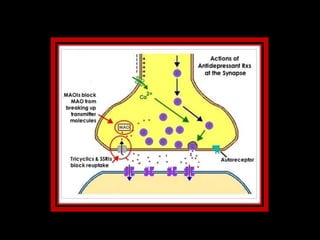
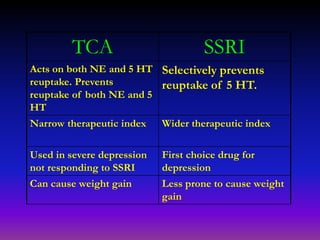
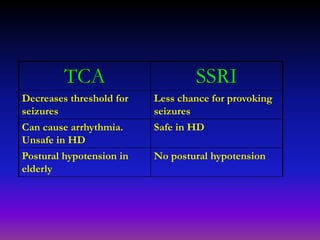
This document discusses antidepressants and their mechanisms and uses. It first outlines several hypotheses for the causes of depression, including reduced levels of neurotransmitters like serotonin, norepinephrine, and dopamine. It then describes the types of antidepressants, focusing on tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs). TCAs act on both serotonin and norepinephrine, while SSRIs only target serotonin. The document contrasts TCAs and SSRIs, noting that TCAs have a narrower therapeutic index and greater side effects like dry mouth and arrhythmias, while SSRIs have fewer side effects and a wider safety margin. Finally, it lists several approved indications