Downloaded 127 times
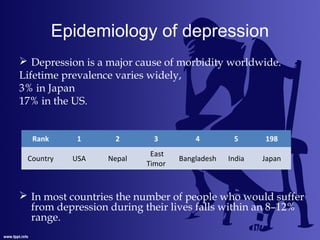



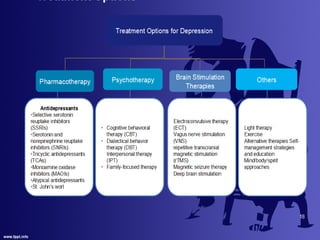




This document provides an overview of anti-depression including definitions, epidemiology, etiology, hypotheses, symptoms, diagnosis, and antidepressants. It defines depression according to the WHO as a common mental disorder characterized by sadness and loss of interest. It notes the lifetime prevalence varies from 3-17% depending on country, and is higher in women. Several hypotheses for the etiology of depression are discussed related to neurotransmitters, receptors, and neuroendocrine factors. Common symptoms and diagnosis criteria from the DSM-V are outlined. Finally, it describes several classes of antidepressants including TCAs, MAOIs, SSRIs, and SNRIs and discusses their mechanisms of action, advantages/disadvantages, side



































































