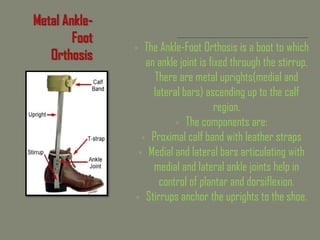
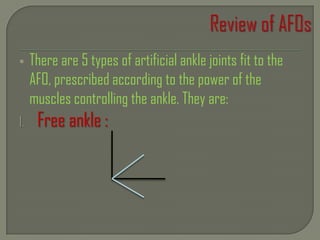
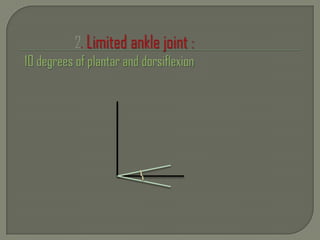
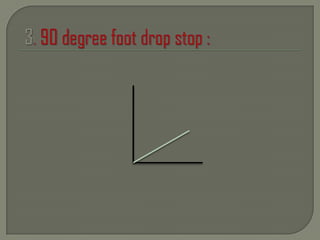
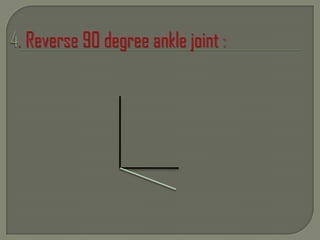
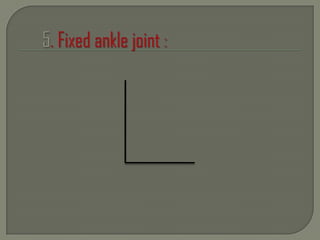
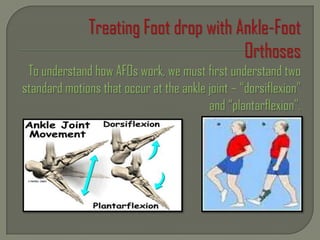
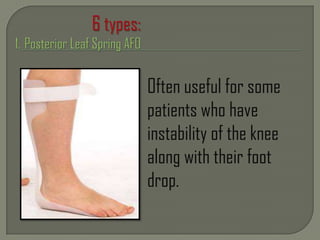
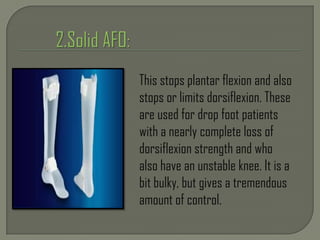
Ankle-foot orthoses (AFOs) are external devices that attach to the lower leg and foot to improve function by controlling motion and providing support. The main components are a calf band, medial and lateral bars that articulate with ankle joints, and a stirrup that anchors to the shoe. There are 5 types of artificial ankle joints prescribed according to muscle strength: free ankle, dorsiflexion stop, plantarflexion stop, fixed dorsiflexion stop, and fixed hinge. AFOs are used to treat drop foot and other conditions involving muscle weakness, deformities, or instability by maintaining proper foot and ankle positioning during gait.



























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









