Downloaded 702 times



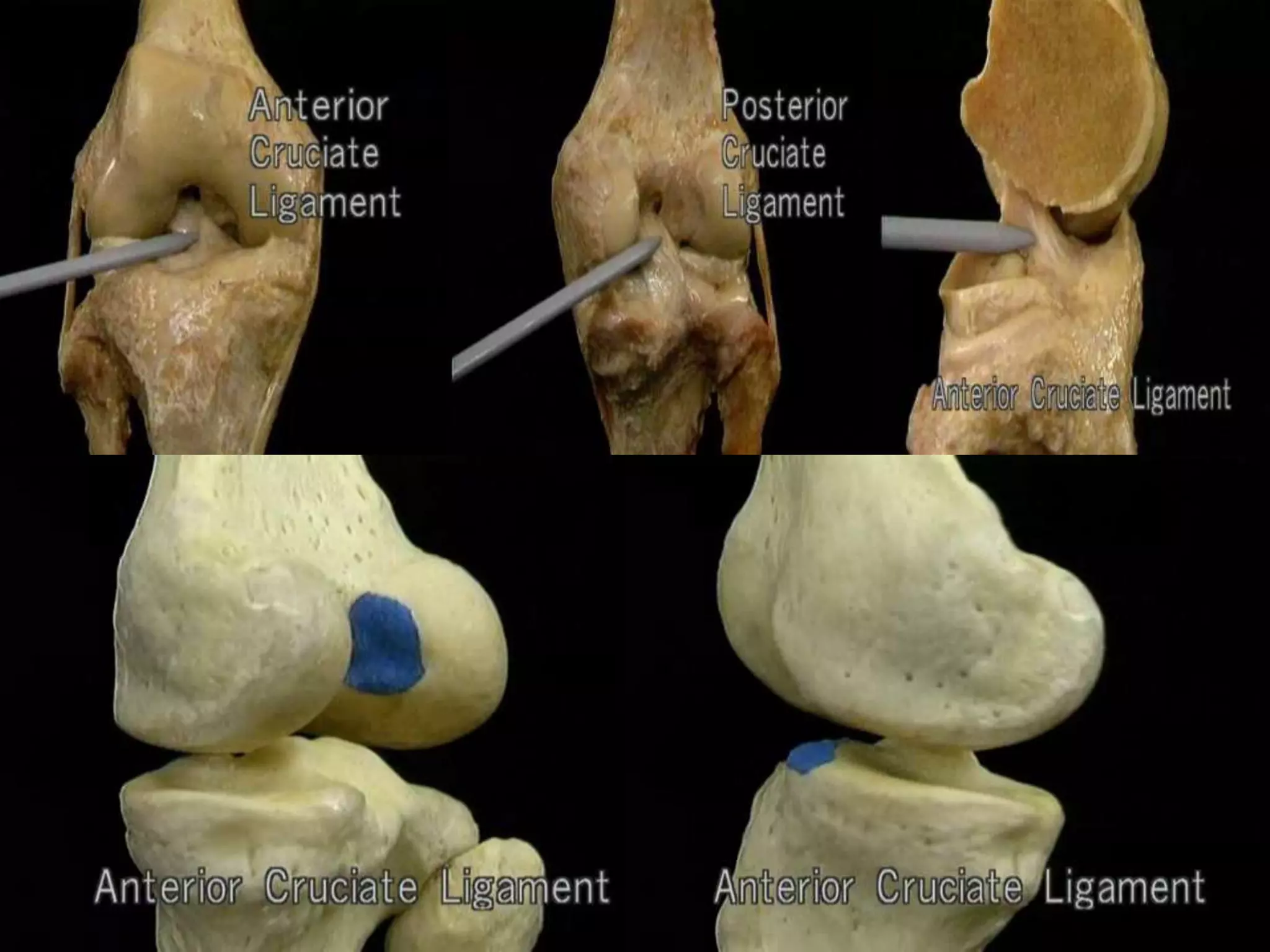




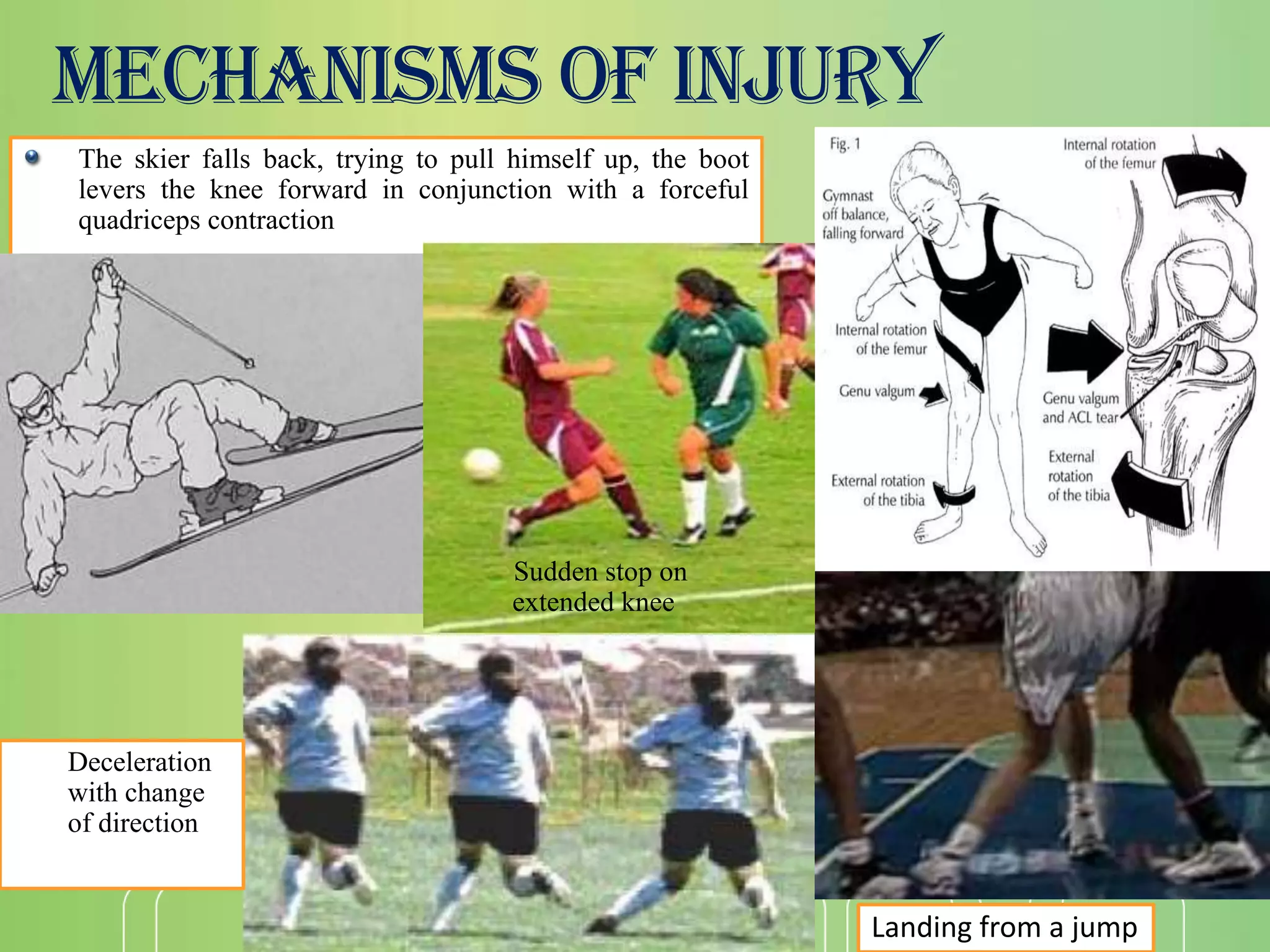























































- The ACL originates on the lateral femoral condyle and inserts on the tibia, providing primary stability to prevent anterior tibial translation. - Most ACL tears are non-contact injuries involving sudden deceleration, change of direction, or landing from a jump with the knee near full extension. - Physical exam includes Lachman, anterior drawer, and pivot shift tests to assess knee stability. MRI is used to confirm ACL tear. - Treatment options include conservative rehab for partial or low-grade tears or ACL reconstruction surgery using grafts like patellar tendon or hamstring tendons fixed with interference screws. Post-op rehab emphasizes early range of motion and weight bearing.