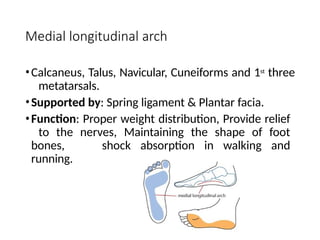
Medial longitudinal arch
•Calcaneus,Talus, Navicular, Cuneiforms and 1st
three
metatarsals.
•Supported by: Spring ligament & Plantar facia.
•Function: Proper weight distribution, Provide relief
to the nerves, Maintaining the shape of foot
bones, shock absorption in walking and
running.
6.
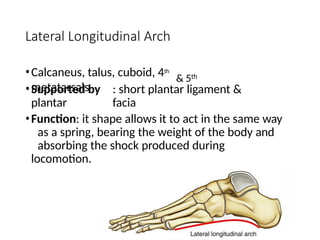
Lateral Longitudinal Arch
&5th
•Calcaneus, talus, cuboid, 4th
metatarsals
•Supported by : short plantar ligament &
plantar facia
•Function: it shape allows it to act in the same way
as a spring, bearing the weight of the body and
absorbing the shock produced during
locomotion.
7.
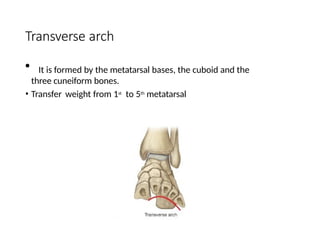
Transverse arch
• Itis formed by the metatarsal bases, the cuboid and the
three cuneiform bones.
• Transfer weight from 1st
to 5th
metatarsal
Introduction
• A lowerlimb orthosis is an external device applied/attached to the
lower body segment to:
• improve function by controlling motion,
• providing support through stabilizing gait,
• reducing pain through transferring load/weight to another area,
• correcting flexible deformities and
• preventing progression of fixed deformities
10.
Foot Orthosis
According tothe Atlas of Orthoses and Assistive Devices:
• Foot orthoses (FO) are like the tires on an automobile. They provide a
critical, biomechanical contact point for the human body, and they
can be helpful to correct problems in the foot, knee, hip, and spine.
• An Orthosis is a single device, a group of them are referred to as
orthoses.
• An Orthosis is basically a mechanical device fitted to the body to
maintain it in an anatomical or functional position.
11.
Foot Orthosis
• Footorthoses have proven to be effective for conservative
management of various pathologies.
• Pathologies of the lower limb can be caused by abnormal
biomechanics such as irregular foot structure and alignment, leading
to inadequate support.
Symptoms
• The mostcommon symptom of flat feet is pain in the feet. This can
occur as a result of strained muscles and connecting ligaments.
• Abnormal stresses on the knee and hip may result in pain in these
joints. These stresses are likely if the ankles turn inward.
• Pain most commonly affects the following parts of the body:
inside ankle, alongside possible swelling,arch of the foot,
calf
muscles, knee, hip, lower back, lower legs
• Flat feet can also cause an uneven distribution of body weight. This
may result in shoes tearing down unevenly or more quickly than
usual, especially on one side, which can lead to further injuries.
14.
Causes
• Flat feetare related to the tissues and bones in your feet and lower
legs.
• The condition is normal in babies and toddlers because it takes time
for the tendons to tighten and form an arch. In rare cases, the bones
in a child’s feet become fused, causing pain.
• You’re more likely to have flat feet if the condition runs in your family.
If you’re highly athletic and physically active, your risk is higher due
to the possibility of foot and ankle injuries.
• Older people who are prone to falls or physical injury are also more
at risk. People with diseases that affect the muscles — for example,
cerebral palsy — also have an increased risk.
• Other risk factors include having obesity and diabetes mellitus.
15.
Types of footOrthosis
• Soft Foot Orthosis
• Semi Rigid Foot Orthosis
• Rigid Foot Orthosis
• UCBL
• Supra Malleolar orthosis- SMO
16.
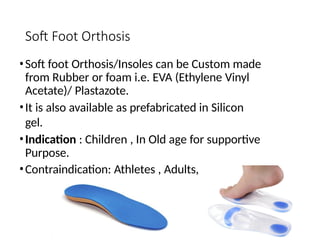
Soft Foot Orthosis
•Softfoot Orthosis/Insoles can be Custom made
from Rubber or foam i.e. EVA (Ethylene Vinyl
Acetate)/ Plastazote.
•It is also available as prefabricated in Silicon
gel.
•Indication : Children , In Old age for supportive
Purpose.
•Contraindication: Athletes , Adults,
17.
Semi-Rigid Foot Orthosis
•Semi-Rigid Foot Orthosis/Insole can be Custom made from Crock or
the combination of EVA with Crock.
• It is also Available in Prefabricated.
• Indications: Athletes, person with High activity level, Children, adults,
Old age.
18.
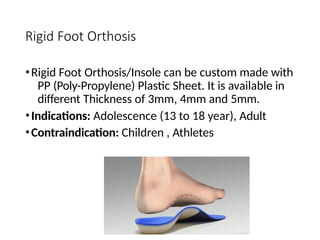
Rigid Foot Orthosis
•RigidFoot Orthosis/Insole can be custom made with
PP (Poly-Propylene) Plastic Sheet. It is available in
different Thickness of 3mm, 4mm and 5mm.
•Indications: Adolescence (13 to 18 year), Adult
•Contraindication: Children , Athletes
19.
UCBL
•The UCBL wasdeveloped in 1967 at the University of
California Biomechanics Laboratory or University
of California at Berkeley Laboratory.
• The UCBL insole/shoe insert is considered a maximum
control foot Orthosis.
• It was named after the Laboratory where it was
researched and developed.
• It is a rigid foot Orthosis used to correct and/or stabilize a
flexible foot deformity.
20.
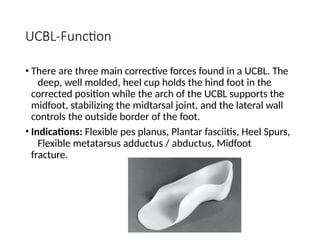
UCBL-Function
• There arethree main corrective forces found in a UCBL. The
deep, well molded, heel cup holds the hind foot in the
corrected position while the arch of the UCBL supports the
midfoot, stabilizing the midtarsal joint, and the lateral wall
controls the outside border of the foot.
• Indications: Flexible pes planus, Plantar fasciitis, Heel Spurs,
Flexible metatarsus adductus / abductus, Midfoot
fracture.
21.
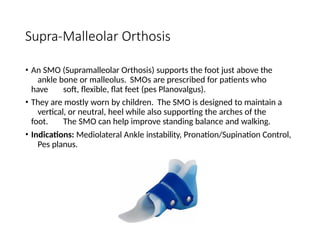
Supra-Malleolar Orthosis
• AnSMO (Supramalleolar Orthosis) supports the foot just above the
ankle bone or malleolus. SMOs are prescribed for patients who
have soft, flexible, flat feet (pes Planovalgus).
• They are mostly worn by children. The SMO is designed to maintain a
vertical, or neutral, heel while also supporting the arches of the
foot. The SMO can help improve standing balance and walking.
• Indications: Mediolateral Ankle instability, Pronation/Supination Control,
Pes planus.
Ankle Foot Orthosis
•Ankle-foot orthoses (AFOs) control the alignment and motion of the
foot and ankle and thereby affect the entire body.
• They are less expensive, more cosmetically acceptable, and more
energy efficient than more extensive bracing.
• In addition, they may enable the patient to achieve the
same functional goals as would be possible with KAFOs and
higher Orthoses
24.
AFO- Indications
• AnkleFoot Orthosis is prescribed for:
1. Muscle weakness effecting the ankle and subtalar joint.
2. Prevention and correction of deformities of ankle and foot
3. Reduction in appropriate weight bearing forces
- Dorsiflexors paralysis
- Ankle foot paralysis
- Spasticity
- Limited weight bearing
25.
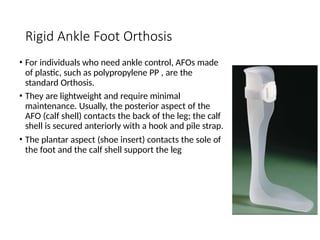
Rigid Ankle FootOrthosis
• For individuals who need ankle control, AFOs made
of plastic, such as polypropylene PP , are the
standard Orthosis.
• They are lightweight and require minimal
maintenance. Usually, the posterior aspect of the
AFO (calf shell) contacts the back of the leg; the calf
shell is secured anteriorly with a hook and pile strap.
• The plantar aspect (shoe insert) contacts the sole of
the foot and the calf shell support the leg
26.
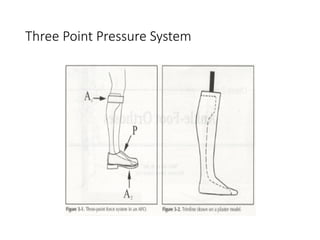
Three point PressureSystem
• An AFO applies a three-point pressure system to the
limb.
• The correcting, anteriorly directed force (A1) is located at
the calf shell and is opposed by a distal,
posteriorly directed force (P) on the dorsum of the
foot from the shoe and an ankle strap, superiorly
directed force (A2) supplied by the shoe sole and
insert (Figure 3-1).
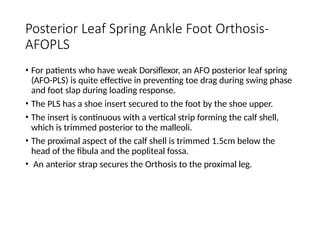
Posterior Leaf SpringAnkle Foot Orthosis-
AFOPLS
• For patients who have weak Dorsiflexor, an AFO posterior leaf spring
(AFO-PLS) is quite effective in preventing toe drag during swing phase
and foot slap during loading response.
• The PLS has a shoe insert secured to the foot by the shoe upper.
• The insert is continuous with a vertical strip forming the calf shell,
which is trimmed posterior to the malleoli.
• The proximal aspect of the calf shell is trimmed 1.5cm below the
head of the fibula and the popliteal fossa.
• An anterior strap secures the Orthosis to the proximal leg.
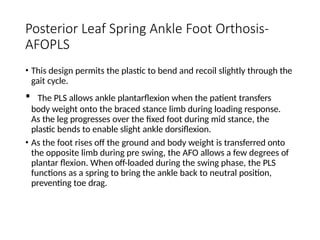
Posterior Leaf SpringAnkle Foot Orthosis-
AFOPLS
• This design permits the plastic to bend and recoil slightly through the
gait cycle.
• The PLS allows ankle plantarflexion when the patient transfers
body weight onto the braced stance limb during loading response.
As the leg progresses over the fixed foot during mid stance, the
plastic bends to enable slight ankle dorsiflexion.
• As the foot rises off the ground and body weight is transferred onto
the opposite limb during pre swing, the AFO allows a few degrees of
plantar flexion. When off-loaded during the swing phase, the PLS
functions as a spring to bring the ankle back to neutral position,
preventing toe drag.
31.
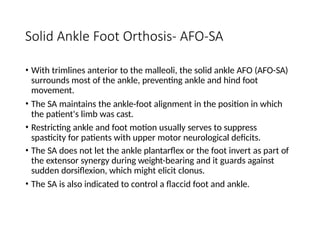
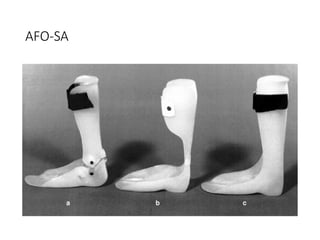
Solid Ankle FootOrthosis- AFO-SA
• With trimlines anterior to the malleoli, the solid ankle AFO (AFO-SA)
surrounds most of the ankle, preventing ankle and hind foot
movement.
• The SA maintains the ankle-foot alignment in the position in which
the patient's limb was cast.
• Restricting ankle and foot motion usually serves to suppress
spasticity for patients with upper motor neurological deficits.
• The SA does not let the ankle plantarflex or the foot invert as part of
the extensor synergy during weight-bearing and it guards against
sudden dorsiflexion, which might elicit clonus.
• The SA is also indicated to control a flaccid foot and ankle.
Solid Ankle FootOrthosis- AFO-SA
• The SA will resist a hyperextended knee such as may be
present in the patient who compensates for quadriceps
weakness by forcing the knee to yield into
hyperextension. The proximal portion of the calf shell
provides an anteriorly directed force near the knee to
restrain hyperextension, and the distal portion of the
calf shell blocks plantar and dorsiflexion
34.
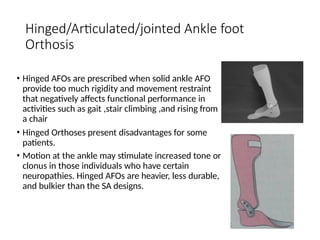
Hinged/Articulated/jointed Ankle foot
Orthosis
•Hinged AFOs are prescribed when solid ankle AFO
provide too much rigidity and movement restraint
that negatively affects functional performance in
activities such as gait ,stair climbing ,and rising from
a chair
• Hinged Orthoses present disadvantages for some
patients.
• Motion at the ankle may stimulate increased tone or
clonus in those individuals who have certain
neuropathies. Hinged AFOs are heavier, less durable,
and bulkier than the SA designs.
35.
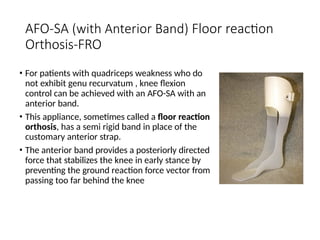
AFO-SA (with AnteriorBand) Floor reaction
Orthosis-FRO
• For patients with quadriceps weakness who do
not exhibit genu recurvatum , knee flexion
control can be achieved with an AFO-SA with an
anterior band.
• This appliance, sometimes called a floor reaction
orthosis, has a semi rigid band in place of the
customary anterior strap.
• The anterior band provides a posteriorly directed
force that stabilizes the knee in early stance by
preventing the ground reaction force vector from
passing too far behind the knee
36.
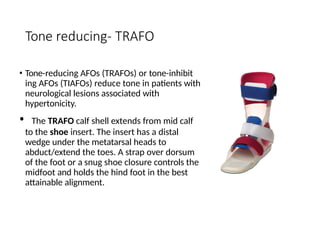
Tone reducing- TRAFO
•Tone-reducing AFOs (TRAFOs) or tone-inhibit
ing AFOs (TIAFOs) reduce tone in patients with
neurological lesions associated with
hypertonicity.
• The TRAFO calf shell extends from mid calf
to the shoe insert. The insert has a distal
wedge under the metatarsal heads to
abduct/extend the toes. A strap over dorsum
of the foot or a snug shoe closure controls the
midfoot and holds the hind foot in the best
attainable alignment.
37.
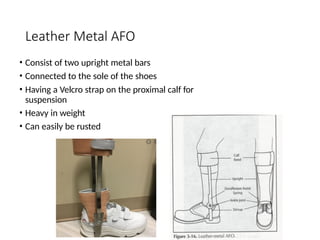
Leather Metal AFO
•Consist of two upright metal bars
• Connected to the sole of the shoes
• Having a Velcro strap on the proximal calf for
suspension
• Heavy in weight
• Can easily be rusted
38.
Weight relieving AFO
•PTB brace in case of tibial fracture
to off load weight from the
fractured area.
39.
Contracture reducing AFO
•The specialized Orthosis/brace is use to control and release the
Achilles tightness along with physiotherapy.
• Usually worn at night.
• The medial and lateral straps is use to dorsiflex the foot and prevent
planter flexion.
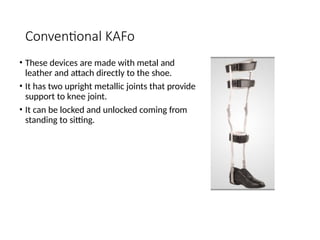
Conventional KAFo
• Thesedevices are made with metal and
leather and attach directly to the shoe.
• It has two upright metallic joints that provide
support to knee joint.
• It can be locked and unlocked coming from
standing to sitting.
43.
Thermoplastic KAFOs
• Theseare custom made Knee ankle foot
orthosis made from Polypropylene PP sheet .
• The process of fabrication contains Casting,
modification, molding cutting and finishing.
• These are light weighted Orthosis easy to
carry by patients.
• It consists of two Side bars (knee joints)
which use to locking and un-locking of knee
joint that helps in walking and sitting.
• 2 straps on thigh and 2 straps on shin are use
for suspension purposes which allows
correction as well
44.
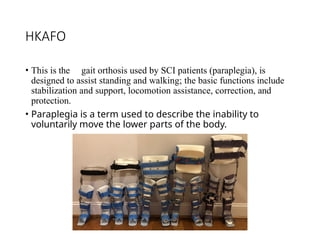
HKAFO
• This isthe gait orthosis used by SCI patients (paraplegia), is
designed to assist standing and walking; the basic functions include
stabilization and support, locomotion assistance, correction, and
protection.
• Paraplegia is a term used to describe the inability to
voluntarily move the lower parts of the body.