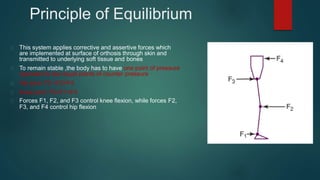
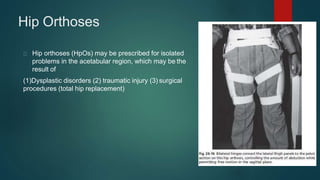
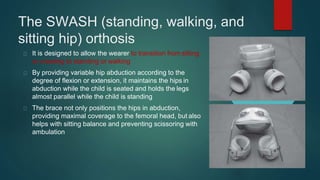
An HKAFO is an orthosis that stabilizes the hip, knee, and ankle. It consists of an AFO connected to thigh sections and a pelvic band. The orthosis applies corrective forces at the skin surface that are transmitted through soft tissues to bones. Forces are balanced at joints to control movement. HKAFOs assist with gait and decrease weight bearing in conditions like paraplegia. Reciprocating gait orthoses use cables to induce reciprocal hip flexion/extension between sides, enabling paraplegic ambulation. Hip orthoses control movement after injuries or surgeries. Pediatric hip orthoses treat developmental dysplasia of the hip and cerebral palsy, maintaining hip ab









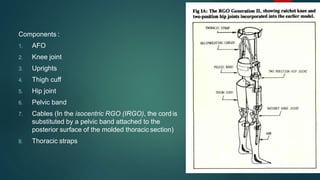
![Reciprocal Gait Orthosis (RGO)
A reciprocating gait orthosis (RGO) is
an HKAFO that uses a mechanical
system that connects the two sides of
the brace by
1. Isocentric bar (IRGO)
2. Double cable (LSU RGO from
Louisiana State University)
3. Single push/pull cable system
(advanced RGO [ARGO] )](https://image.slidesharecdn.com/hiporthosis-220822074743-27134cd0/85/hip-orthosis-pptx-15-320.jpg)







































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
