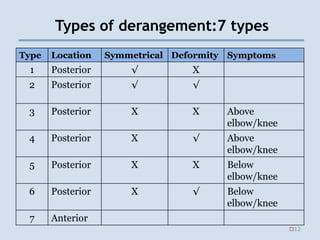
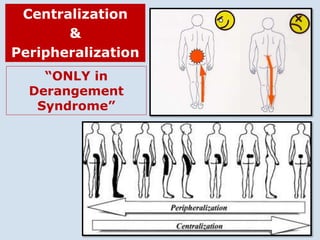
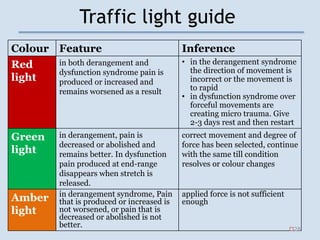
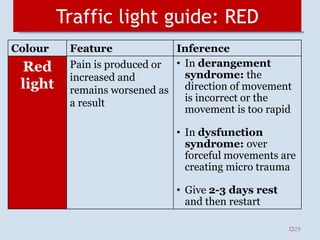
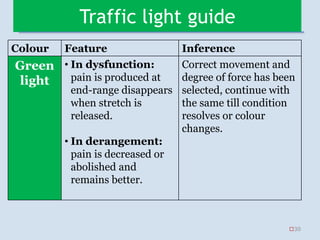
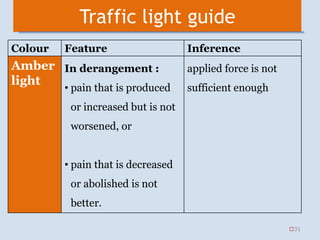

The document outlines the McKenzie method of spinal therapy, detailing three syndromes: postural, dysfunction, and derangement, along with their clinical features. It emphasizes the importance of repeated movement testing to identify syndromes, predict treatment outcomes, and guide management strategies. Additionally, it introduces a traffic light guide for assessing movement responses during treatment.























































































