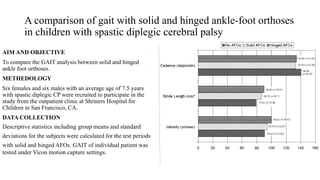
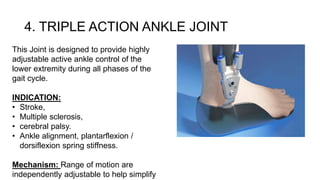
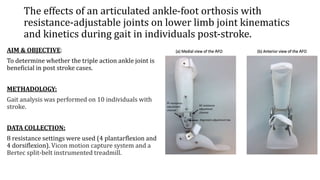
The document outlines various types of orthotic ankle joints used in rehabilitation, detailing their mechanical functions, indications, and effects on gait. It compares the performance of different ankle-foot orthoses (AFOs) in patients with conditions like stroke and cerebral palsy, highlighting the benefits of adjustable joints. Findings suggest that while certain AFOs improve ankle motion and stability, preferences may vary based on factors like weight and functionality.