Downloaded 983 times
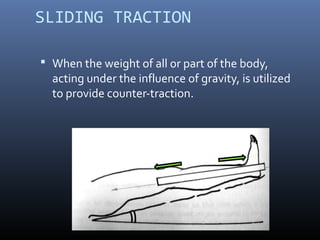


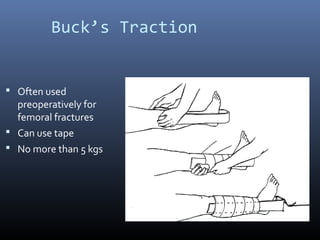

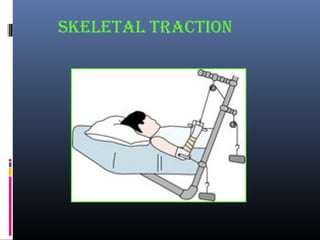
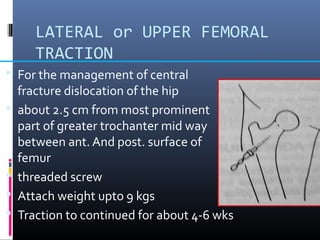

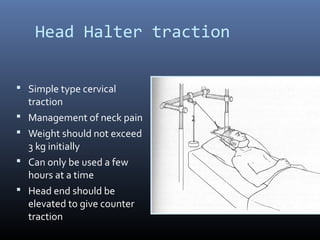


This document discusses different types of traction used in orthopedics. It defines traction as applying a stretching force to parts of the body. Traction is used to reduce fractures and dislocations, immobilize painful joints, prevent deformity, and correct soft tissue contractures. The document describes different methods of skin traction including Buck's traction and Bryant's traction, as well as skeletal traction using pins in the femur, tibia, or calcaneus. Complications of traction include infection, nerve injury, and distraction at the fracture site.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







