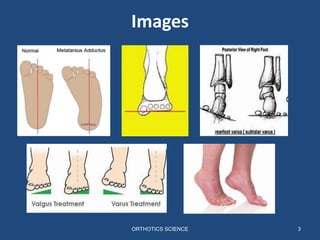
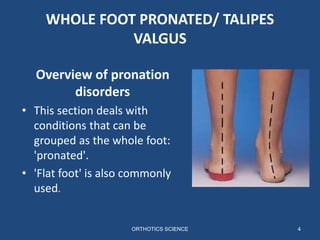
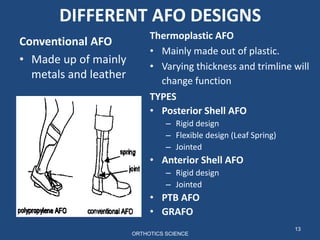
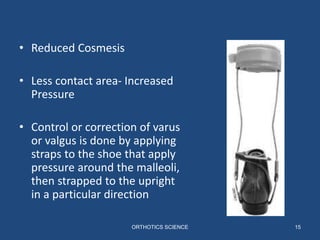
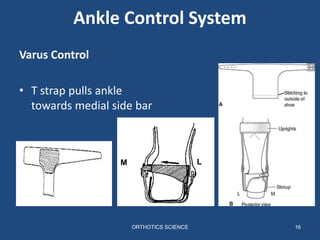
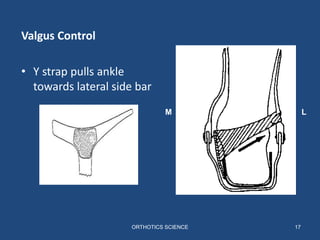
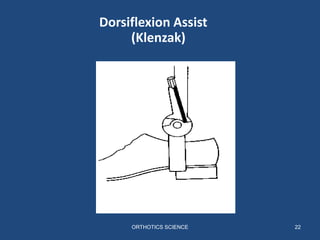
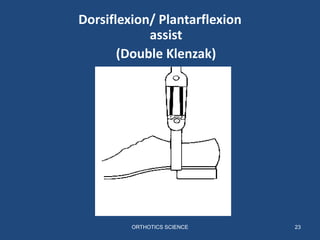
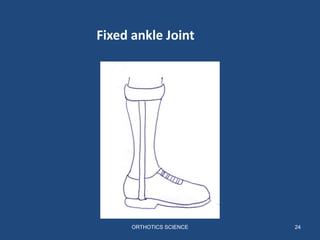
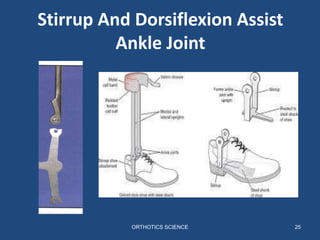
This document discusses orthotics for abnormalities in the coronal, sagittal, and transverse planes of the foot. It focuses on pronated and supinated foot types, describing their key features. Different types of ankle-foot orthoses are outlined, including conventional metal/leather designs, thermoplastic designs, and different variations for posterior, anterior, and PTB styles. Conventional AFO designs are described in more detail, explaining how they use straps on the shoe to provide varus or valgus control and different types of ankle joints for motion restriction or assistance. Complications of bracing are also listed.