INTRODUCTION
Aneurysm isan abnormal bulge in the wall of an artery
Aneurysm 15.000 deaths yearly, 10th
leading causes
Atherosclerosis plaque formation and rupture can increase the risk of
aneurysm
Aortic aneurysms are balloon-like bulges that occur in the aorta, the
main artery carrying oxygen-rich blood to your body.
The aorta has thick walls that stand up to normal blood pressure.
However, certain medical problems, genetic conditions, and trauma
can damage or weaken these walls. The force of blood pushing against
the weakened or injured walls can cause an aneurysm.
4.
Definition
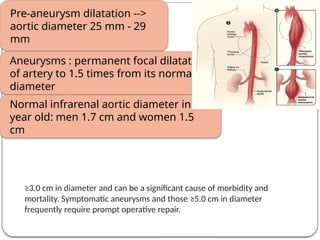
Pre-aneurysm dilatation -->
aorticdiameter 25 mm - 29
mm
Aneurysms : permanent focal dilatation
of artery to 1.5 times from its normal
diameter
Normal infrarenal aortic diameter in 50
year old: men 1.7 cm and women 1.5
cm
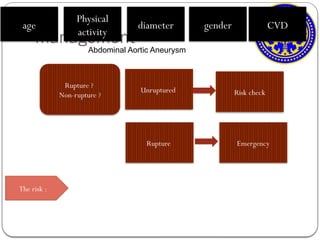
≥3.0 cm in diameter and can be a significant cause of morbidity and
mortality. Symptomatic aneurysms and those ≥5.0 cm in diameter
frequently require prompt operative repair.
5.
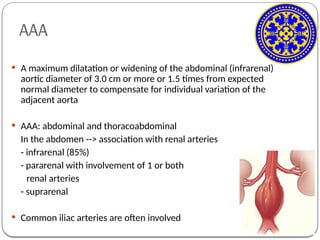
AAA
A maximumdilatation or widening of the abdominal (infrarenal)
aortic diameter of 3.0 cm or more or 1.5 times from expected
normal diameter to compensate for individual variation of the
adjacent aorta
AAA: abdominal and thoracoabdominal
In the abdomen --> association with renal arteries
- infrarenal (85%)
- pararenal with involvement of 1 or both
renal arteries
- suprarenal
Common iliac arteries are often involved
Epidemiology
AAA
But AAA is
decreased
Olderpatients (65-80 years) --> 2.2%
Prevalence : men 4-8% and women 1-2%
Prevalence Aortic aneurysm is increased,
From 15,000 to 13,000 deaths yearly
In 2000 --> 10th leading cause of death in USA
TAA - 6 cases per 100,000 person-years
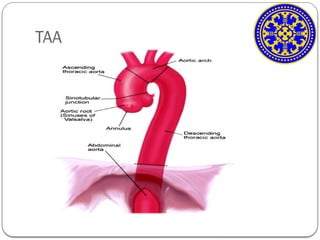
8.
Etiology
• Ascending thoracicaortic aneurysm
• Histologically appear as smooth muscle dropout and
elastic fiber degeneration
• Leads to weakening of aortic wall, causing aortic
dilatation and aneurysm formation
Cystic medial degeneration
• In young patients
• Heritable disorder
• Mutation in one of the genes for fibrilin-1
Marfan Syndrome
9.
• Heritable
• Ascendingthoracic aortic aneurysm
• Aortic regurgitation aortic valve become
stiff and not opening well heart pumping
harder aorta dilatation
Bicuspid Aortic valve
• Aneurysm of descending thoracic aorta
• Aneurysm of abdominal aorta
Atherosclerosis
10.
• In secondphase of disease, spirochetes infect the aortic
media
• Destruction of collagen and elastic tissue aorta dilatation
Syphilis
• Takayasu’s arteritis
• In young women
Aortic Arteritis
Aortic Dissection
• distinct saccular
Trauma
11.
SYMPTOMS
Sudden severeback or abdominal pain, hypotension, and a pulsa_x0002_tile
abdominal mass. Patients may also present with syncope or pain that localizes
to the flank, groin, hip, or abdomen.
Half of patients with a rupturing aneurysm describe a ripping or tearing pain
that is severe and abrupt in onset.
Difficult or painful swallowing if the aneurysm pushes on your esophagus, the
tube that connects your mouth and your stomach
Difficulty breathing if it pushes on your trachea, or windpipe
Feeling full after not eating very much
Hoarseness
Pain in the neck, jaw, back, chest, stomach area or shoulder, depending on
where the aneurysm is located
A pulsating or throbbing feeling in your stomach area
Shortness of breath if the aneurysm presses on your lung
Swelling of the face, neck, or arms if the aneurysm pushes on the superior vena
cava, the main vein returning blood from your upper body to your heart
Light-headedness,Rapid heart rate,Sudden, severe pain
12.
RISK FACTORS
• Abdominalaortic aneurysm
Smoking
• Old age
• Men tend to get abdominal aortic aneurysm at younger age
compared to women
Age
Hypertension
Hyperlipidemia
• Men > women
• Women with abdominal aortic aneurysm are likely to have family history
of the disorder
Gender
13.
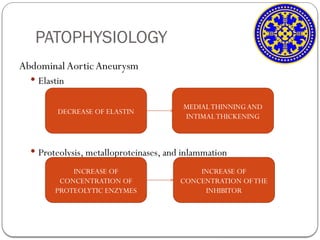
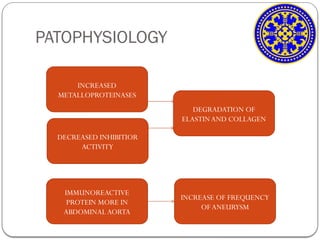
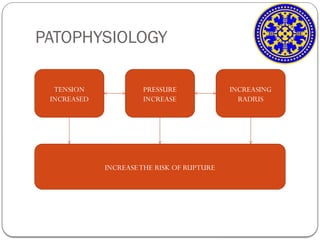
PATOPHYSIOLOGY
Abdominal AorticAneurysm
Elastin
Proteolysis, metalloproteinases, and inlammation
DECREASE OF ELASTIN
MEDIALTHINNINGAND
INTIMALTHICKENING
INCREASE OF
CONCENTRATION OF
PROTEOLYTIC ENZYMES
INCREASE OF
CONCENTRATION OFTHE
INHIBITOR
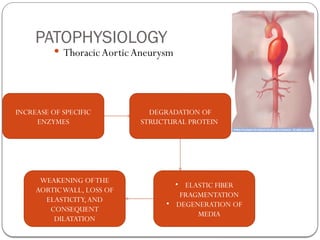
PATOPHYSIOLOGY
ThoracicAortic Aneurysm
INCREASEOF SPECIFIC
ENZYMES
DEGRADATION OF
STRUCTURAL PROTEIN
WEAKENING OFTHE
AORTICWALL, LOSS OF
ELASTICITY,AND
CONSEQUENT
DILATATION
• ELASTIC FIBER
FRAGMENTATION
• DEGENERATION OF
MEDIA
Sign and Symptom
AbdominalAorticAneurysm
• Pain in the abdomen
• Pain radiating to lower
back
• Nausea and vomiting
• Constipation
• Light-headedness
ThoracicAortic Aneurysms
• Asymptomatic
• Pain in jaw, neck and chest
• Pressure on trachea:
dyspnea and cough
• Pain while swelling
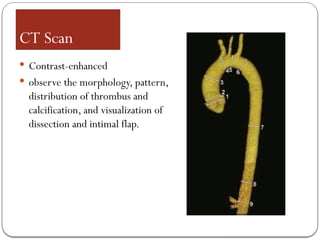
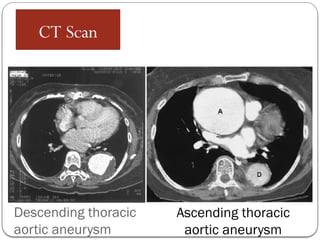
CT Scan
Contrast-enhanced
observe the morphology, pattern,
distribution of thrombus and
calcification, and visualization of
dissection and intimal flap.
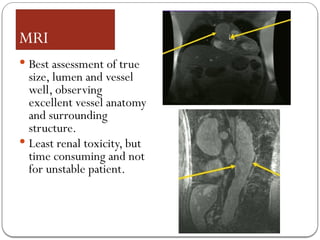
MRI
Best assessmentof true
size, lumen and vessel
well, observing
excellent vessel anatomy
and surrounding
structure.
Least renal toxicity, but
time consuming and not
for unstable patient.
25.
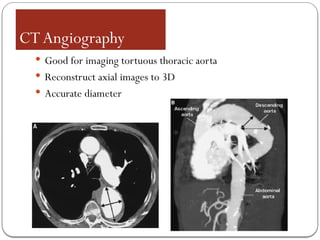
CTAngiography
Good forimaging tortuous thoracic aorta
Reconstruct axial images to 3D
Accurate diameter
26.
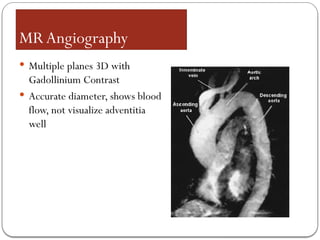
MRAngiography
Multiple planes3D with
Gadollinium Contrast
Accurate diameter, shows blood
flow, not visualize adventitia
well
27.
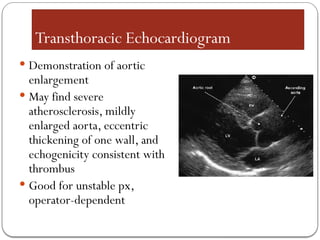
Transthoracic Echocardiogram
Demonstrationof aortic
enlargement
May find severe
atherosclerosis, mildly
enlarged aorta, eccentric
thickening of one wall, and
echogenicity consistent with
thrombus
Good for unstable px,
operator-dependent
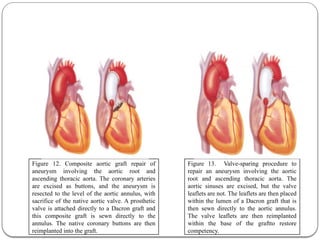
Figure 13. Valve-sparingprocedure to
repair an aneurysm involving the aortic
root and ascending thoracic aorta. The
aortic sinuses are excised, but the valve
leaflets are not. The leaflets are then placed
within the lumen of a Dacron graft that is
then sewn directly to the aortic annulus.
The valve leaflets are then reimplanted
within the base of the graftto restore
competency.
Figure 12. Composite aortic graft repair of
aneurysm involving the aortic root and
ascending thoracic aorta. The coronary arteries
are excised as buttons, and the aneurysm is
resected to the level of the aortic annulus, with
sacrifice of the native aortic valve. A prosthetic
valve is attached directly to a Dacron graft and
this composite graft is sewn directly to the
annulus. The native coronary buttons are then
reimplanted into the graft.
36.
Ascending Aortic
Aneurysms
Surgery isindicated in patients who have aortic root
aneurysm, with maximal aortic diameter ≥50 mm for
patients with Marfan syndrome.
Surgery should be considered in patients who have aortic root
aneurysm, with maximal ascending aortic diameters:
≥45 mm for patients with Marfan syndrome with risk
factors.
≥50 mm for patients with bicuspid valve with risk factors
≥55 mm for other patients with no elastopathy
37.
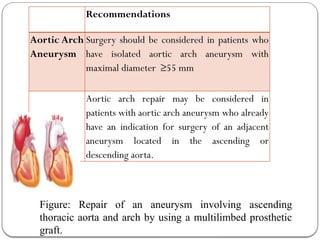
Recommendations
Aortic Arch
Aneurysm
Surgery shouldbe considered in patients who
have isolated aortic arch aneurysm with
maximal diameter ≥55 mm
Aortic arch repair may be considered in
patients with aortic arch aneurysm who already
have an indication for surgery of an adjacent
aneurysm located in the ascending or
descending aorta.
Figure: Repair of an aneurysm involving ascending
thoracic aorta and arch by using a multilimbed prosthetic
graft.
38.
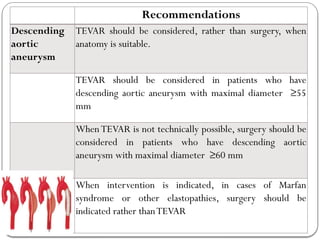
Recommendations
Descending
aortic
aneurysm
TEVAR should beconsidered, rather than surgery, when
anatomy is suitable.
TEVAR should be considered in patients who have
descending aortic aneurysm with maximal diameter ≥55
mm
WhenTEVAR is not technically possible, surgery should be
considered in patients who have descending aortic
aneurysm with maximal diameter ≥60 mm
When intervention is indicated, in cases of Marfan
syndrome or other elastopathies, surgery should be
indicated rather thanTEVAR
39.
Prevention of AorticAneurysm
• Preventive ofAortic Aneurysm is to modified its risk factors.
If your parents and close - related family are considered had Aortic
Aneurysm before, it wise to avoid:1,2
Smoking
Hyperlipidemia
Hypertension control
Sedentary lifestyle
References
1. Sakalihasan N, Limet R, Dewafe OD.Abdominal AorticAneurysm. Journal of Lancet.Vol 365; 2005.Accessed from www.thelancet.com (17 April 2015)
2. Fauci AS, et al. Harrison’s Principles of Internal Medicine. 17th
ed. McGraw-Hills Companies; United States ofAmerica, 2008.
40.
PROGNOSIS
For patients whosuffer rupture of an AAA before hospital arrival, the
prognosis is guarded. The survival rate for patients who can reach the
emergency department at the time is about 1% per minute, but it will
higher (about more than 50%) for those who don’t
In patients undergoing surgery for descending thoracic aortic aneurysms,
the operative mortality rate for all cases (emergency or elective) averaged
11%. Elective surgical repair of descending thoracic aortic aneurysms is
also associated with a mortality rate ranging from 5% to 14%. Risk factors
for early mortality and morbidity included emergency operation,
congestive heart failure, advanced age, and atherosclerotic etiology.
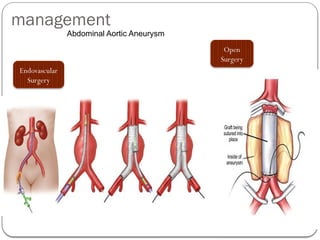
Complication After Abdominal
AorticAneurysm Repair
After Open Repair
(Graft Related
Complications)
• Anastomotic
aneurysms
• graft infection
• Secondary
aortoenteric fistulae
After Open Repair
(Non-graft Related
Complications)
• Sexual dysfuction
Complication After
Endovascular Aortic
Repair
• Endovascular leak
• aortic stent-graft
infection
• kinking, migration and
occlusion
43.
CONCLUSION
Aneurysms arepermanent focal dilatation of artery to 1.5 times from
its normal diameter
AAA will be showed as pain in the abdomen, radiating to back, nausea
and vomiting. TAA are mostly asymptomatic
Abdominal USG is primary method for screening AAA
The treatment will be based on the part of aortic that affected with
aneurysm
It wise to avoid: smoking, hyperlipidemia, hypertention, and sedentary
life
44.
Case 1: ThoracicAortic Aneurysm
Reference: Duru S, Erdem M, Agca E, Kaplan T, Ardic S.Thoracic Aortic Aneurysm: A Rare Case
Report.TurkishThoracic Society. 2013; 14: 78-80
CASE DESCRIPTION
Male, 72 years old admitted to Dept. of Chest Disease with:
ANAMNESIS
1.Chief complaint: back pain for the past two years which is intermittent interscapular
pain independent of position, breathing and exercise.The last pain had been present for
2 months
2.Past history: hypertension for 20 years with an irregular antihypertensive treatment,
he did not have any known genetic disease, no systemic connective tissue disease,
infection, genetic defects, inflammation, or history of trauma
3.Family history: his parents had suffered from hypertension and diabetes
4.Social history: no history of smoking, coughing, weight loss, dyspnoea, dysphagia and
haemoptysis.
45.
PHYSICAL EXAMINATION
1. VitalSign : BP: 140/80 mm Hg, PR: 90 beats/minute, RR: 16 breaths/minute,
T.ax : 36°C
2. Cardiac and other system examinations were normal, but there was a decrease of
breathe sounds in the left infrascapular area in the auscultation
SUPPORTING EXAMINATION
3. CBC, biochemical and serological analyses were normal
4. Normal erythrocyte sedimentation rate of 10 mm/h and a white blood cell count
of 9×109/L
5. High sensitivity C-reactive protein and serum D-dimer levels were found to be
normal
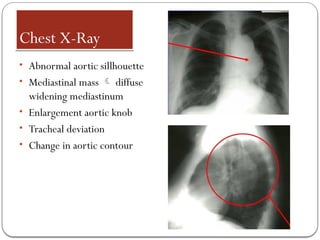
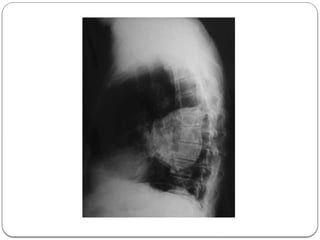
6. Posteroanterior chest X- ray (Figure 1) examination revealed a large left hilar
mass. In addition to a lack of aeration of the lower lobe of the left lung, there was
minimal costophrenic sinus bluntness
48.
SUPPORTING EXAMINATION:
1. Inechocardiographic examination, systolic function was normal (fractional
shortening: 30%, ejection fraction: 65%), there was grade I diastolic dysfunction,
mitral lid E-A velocity: 0.7 m/s, no mitral failure, no valvular regurgitation and
hypertrophy (interventricular septum diastolic diameter: 10 mm).
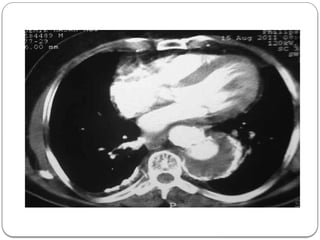
2. Thorax CT scan showed that the mass was located in the proximal part of the
descending aorta, with a diameter of 8 cm, suggesting a saccular aortic aneurysm
3. Defined thrombus material was pressurising the posterior of the oesophagus and the
left atrium. Also, due to compression, atelectasis was seen on the posterobasal
segment of the left lung
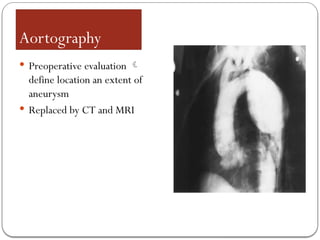
4. Thoracic aortography examination showed an aneurysm located in the proximal part
of the descending aorta with a diameter of 8 cm
5. A large thrombus (6 cm) and atherosclerotic atheroma plaques were shown within
theTAA
50.
TREATMENT FORTHIS PATIENT
Insurgical treatment, under general anaesthesia penetrating to the
femoral artery and using arcus aortagraphy and toracal aortagraphy, an
aneurysm with a diameter of approximately 8 cm was discovered.The
30x120 mm aortic stent graft was applied to the aneurysm. In the
postoperative phase, the patient had no back pain. No complication
was seen; after follow-up and improvement of their general condition,
the patient was discharged from the hospital on postoperative day 15.
51.
CASE DISCUSSION
1. RuptureofTAA and dissections are very rare, despite the very high morbidity and
mortality rates
2. Thoracic aortic aneurysms are usually asymptomatic (about 75%), but pain is
known as the predominant referable symptom in about 17% of patients.
3. Chest pain, back pain, hoarseness due to recurrent laryngeal nerve compression,
difficulty in swallowing due to compression of the oesophagus and shortness of
breath due to the bronchial compression may be seen
4. In aneurysms, smoking history, chronic obstructive pulmonary disease, advanced
age, pain, hypertension, and a diameter of more than 5 cm of the aorta increases
the risk of aortic rupture
5. Nowadays, because of low morbidity, mortality and hospital stay, thoracic
endovascular stent graft surgery, generally under epidural anaesthesia, is the
preferred surgical method in especially oldTAA patients
52.
6. Thoracic endovascularstent graft surgery was applied to this patient
7. The lack of postoperative complications suggests that endovascular stent graft
surgery inTAA without rupture or dissection will diminish mortality rates
8. Despite it’s rare incidence, TAA should not be forgotten in the differential
diagnosis of chronic back pain because early diagnosis diminishes mortality rates
and increases the quality of life for patients.