Downloaded 34 times

![ESC when surgery is indicated ?
The ESC identifies symptomatic heart failure or
echocardiographic signs of poor hemodynamic tolerance
as indicators for surgery associated with echocardiographic
findings of left-sided severe regurgitation, obstruction, or
fistula formation.
If the hemodynamic abnormality is acute and associated with
shock, then emergency surgery is indicated [3].
By the ESC recommendations, surgery should be considered
for native valve aortic or mitral vegetations >10 mm with low
operative risk or for very large vegetations >30 mm](https://image.slidesharecdn.com/infectiveendoecho-210502050344/85/Infective-endocarditis-Echocardiography-22-320.jpg)
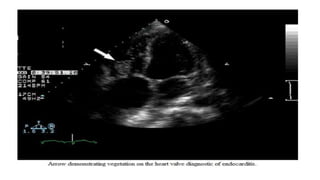
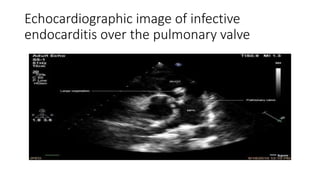

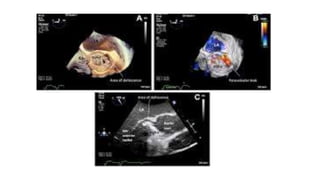
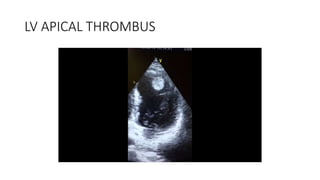
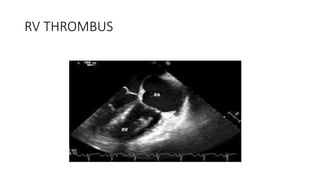


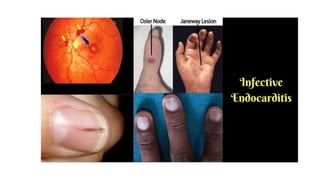
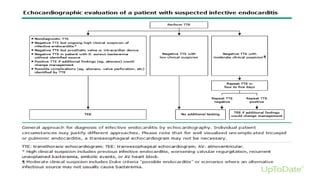
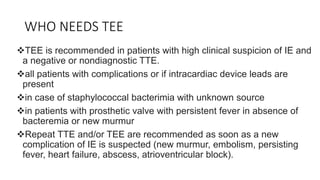
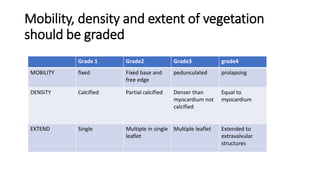
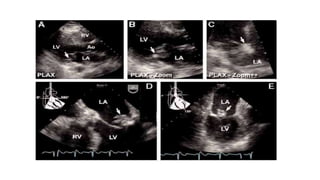
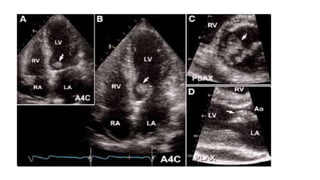
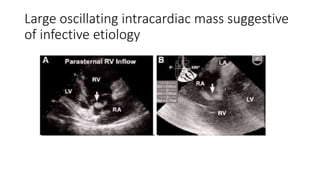
Echocardiography plays a key role in the diagnosis and management of infective endocarditis. It can identify valvular vegetations, abscesses, fistulas and other complications. The presence of an oscillating intracardiac mass or abscess on valves or endocardial surfaces are major echocardiographic criteria for the diagnosis. Transesophageal echocardiography is recommended if transthoracic is nondiagnostic or for complications. Follow up echos are important to monitor vegetation size with treatment and check for complications. Differentiating infective vegetations from other intracardiac masses or artifacts is important.




















































![ivct and ivrt IN CARDIAC CYCLE [Autosaved] .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ivctandivrtautosaved-copy-250829033609-78e4fe1b-thumbnail.jpg?width=640&height=640&fit=bounds)


































