This document discusses thoracic aortic aneurysms. It defines a thoracic aneurysm and notes their locations in the aorta. While less common than abdominal aortic aneurysms, thoracic aneurysms carry a high mortality. They develop due to degradation of the tunica media layer of the aorta. Risk factors include family history, hypertension, smoking, and advancing age. Symptoms vary depending on the location but often include chest or back pain. Imaging such as CT scan is used to diagnose. Management involves medical therapy as well as surgical intervention depending on the location and size of the aneurysm.
DEFINITION:
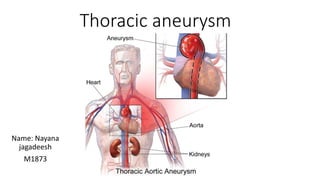
An aortic aneurysm is an enlargement (dilation) of the aorta to greater than 1.5 times normal size.
1)Abdominal aortic aneurysm:
2)Thoracic aortic aneurysm:
1)Hardening of the arteries ( Atherosclerosis).
2)Genetic conditions:
Aortic aneurysms in younger people often have a genetic cause –people who are born with Marfan syndrome.
3)Other medical conditions: Inflammatory conditions ,such as giant cell arteritis.
4)Problems with your hearts aortic valve:
Some times people who have problems with the valve.
5)Untreated infection: Such as syphilis or salmonella, and HIV.
6)Traumatic injury: Rarely ,some people who are injured in falls or motor vehicle crashes develop thoracic aortic aneurysms.
RISK FACTORS-1)Age
2)Male gender
3)Hypertension
4)Coronary artery disease
5)Family history
6)High cholesterol
7)Lower extremity
8)Carotid artery disease.
9)Previous stroke
10)Tobacco use
11)Excess weight.
SIGN & SYMPTOMS-
THORACIC AORTIC ANEURYSM.
•Constant boring pain, which may occur only when the patient is in the supine position.
Dyspnea, cough( parpoxysmal and brassy).
Hoarseness , stridor ,weakness or completer loss of the voice( aphonia).
Dysphagia.
Dilated superficial veins on chest ,neck, neck or arms.
Edematous areas on chest wall.
Cyanosis
Unequal pupils.
1.Patients complaints of “ heart beating” in abdomen when lying down or a feeling of an abdominal mass or abdominal throbbing.
2.Cyanosis and mottling of the toes if aneurysm is associated with thrombus.
DIAGNOSTIC MEASURE-Chest x.ray , CT angiography ( CTA), and transesophageal electrocardiography( TEE) , are done to reveal abnormal widening of the thoracic aorta.
Abdominal aortic aneurysm : Pulsation of pulsatile mass in the middle and upper abdomen , duplex ultrasonography or CTA is used to determine the size ,length and location of the aneurysm.
Dissecting aneurysm : Arteriography ,CTA,TEE duplex ultrasonography and magnetic resonance angiography ( MRA).
COMPLICATION
•Rupture of an aneurysm is the most serious complication.
•If rupture occurs into the retroperitoneal space , bleeding may be controlled by surrounding anatomic structures, preventing exsanguination and death.
MEDICALMANAGEMENT
•The goal of both medical and surgical management is to prevent aneurysm rupture.
•Early detection and prompt treatment are essential .
•Conservative therapy of small asymptomatic AAA’s ( 4-5.5) is the best practice.
This consists of risk factor modification ( ceasing tobacco use , decreasing B.P, optimizing of aneurysm size using ultrasound ,CT, or MRI.
•Growth rates may be lowered with B- adrenergic blocking agents ( eg. Propranolol) , Statins ( eg. Simvastatin) and antibiotics( eg. Doxycycline).
SURGICAL MANAGEMENT-Surgical repair is recommended in patients. with asymptomatic aneurysm 5-5 cm in diameter or larger.
•Surgical procedure are
1)Open aneurysm repair (OAR)
2)Endovascular graft procedure
introduction,
definition
types
causes etc
Management
Routine ultrasound procedures. These procedures will monitor the size and rate of growth of the aneurysm every 6 months to 12 months as part of a "watchful waiting" approach for smaller aneurysms.
Controlling or modifying risk factors. Steps such as quitting smoking, controlling blood sugar if diabetic, losing weight if overweight or obese, and controlling dietary fat intake may help to control the progression of the aneurysm.
Medication. Medication can control factors such as hyperlipidemia (elevated levels of fats and cholesterol in the blood) and/or high blood pressure.
Surgery
Aneurysm open repair. An incision is made to directly visualize and repair the aneurysm. A cylinder-like tube called a graft may be used to repair the aneurysm. Grafts are made of various materials, such as Dacron The open repair is considered the surgical standard for an abdominal aortic aneurysm repair
Endovascular aneurysm repair (EVAR). EVAR is a procedure that requires only small incisions in the groin along with the use of X-ray guidance and specially-designed instruments to repair the aneurysm. With the use of special endovascular instruments and X-ray images for guidance, a stent-graft is inserted via the femoral artery and advanced up into the aorta to the site of the aneurysm.
ANEURYSMS , TYPES AND THERE MANAGEMENT.pptxBipul Thakur
Discussion about different types of Aneurysm, details about Abdominal aorta aneurysm and brief discussion about some important peripheral aneurysms.
Includes approach to different forms of Abdominal aortic aneurysm, its management and complications related to the surgery.
Chronic Stable Angina- Diagnosis & management
By Dr Awadhesh Kumar Sharma
Dr. Awadhesh kumar sharma is a young, diligent and dynamic interventional cardiologist. He did his graduation from GSVM Medical College Kanpur and MD in Internal Medicine from MLB Medical college jhansi. Then he did his superspecilisation degree DM in Cardiology from PGIMER & DR Ram Manoher Lohia Hospital Delhi. He had excellent academic record with Gold medal in MBBS,MD and first class in DM.He was also awarded chief ministers medal in 2009 for his academic excellence by former chief minister of UP Smt Mayawati in 2009.He is also receiver of GEMS international award.He had many national & international publications.He is also in editorial board of international journal- Journal of clinical medicine & research(JCMR).He is also active member of reviewer board of many journals.He is also trainee fellow of American college of cardiology. He is currently working in NABH Approved Gracian Superspeciality Hospital Mohali as Consultant Cardiologist.
Carotid artery disease is commonly seen in association with atherosclerosis and complicate the situation. clearcut guidelines with necessary surgical details are provided in presentations.
DEFINITION:
An aortic aneurysm is an enlargement (dilation) of the aorta to greater than 1.5 times normal size.
1)Abdominal aortic aneurysm:
2)Thoracic aortic aneurysm:
1)Hardening of the arteries ( Atherosclerosis).
2)Genetic conditions:
Aortic aneurysms in younger people often have a genetic cause –people who are born with Marfan syndrome.
3)Other medical conditions: Inflammatory conditions ,such as giant cell arteritis.
4)Problems with your hearts aortic valve:
Some times people who have problems with the valve.
5)Untreated infection: Such as syphilis or salmonella, and HIV.
6)Traumatic injury: Rarely ,some people who are injured in falls or motor vehicle crashes develop thoracic aortic aneurysms.
RISK FACTORS-1)Age
2)Male gender
3)Hypertension
4)Coronary artery disease
5)Family history
6)High cholesterol
7)Lower extremity
8)Carotid artery disease.
9)Previous stroke
10)Tobacco use
11)Excess weight.
SIGN & SYMPTOMS-
THORACIC AORTIC ANEURYSM.
•Constant boring pain, which may occur only when the patient is in the supine position.
Dyspnea, cough( parpoxysmal and brassy).
Hoarseness , stridor ,weakness or completer loss of the voice( aphonia).
Dysphagia.
Dilated superficial veins on chest ,neck, neck or arms.
Edematous areas on chest wall.
Cyanosis
Unequal pupils.
1.Patients complaints of “ heart beating” in abdomen when lying down or a feeling of an abdominal mass or abdominal throbbing.
2.Cyanosis and mottling of the toes if aneurysm is associated with thrombus.
DIAGNOSTIC MEASURE-Chest x.ray , CT angiography ( CTA), and transesophageal electrocardiography( TEE) , are done to reveal abnormal widening of the thoracic aorta.
Abdominal aortic aneurysm : Pulsation of pulsatile mass in the middle and upper abdomen , duplex ultrasonography or CTA is used to determine the size ,length and location of the aneurysm.
Dissecting aneurysm : Arteriography ,CTA,TEE duplex ultrasonography and magnetic resonance angiography ( MRA).
COMPLICATION
•Rupture of an aneurysm is the most serious complication.
•If rupture occurs into the retroperitoneal space , bleeding may be controlled by surrounding anatomic structures, preventing exsanguination and death.
MEDICALMANAGEMENT
•The goal of both medical and surgical management is to prevent aneurysm rupture.
•Early detection and prompt treatment are essential .
•Conservative therapy of small asymptomatic AAA’s ( 4-5.5) is the best practice.
This consists of risk factor modification ( ceasing tobacco use , decreasing B.P, optimizing of aneurysm size using ultrasound ,CT, or MRI.
•Growth rates may be lowered with B- adrenergic blocking agents ( eg. Propranolol) , Statins ( eg. Simvastatin) and antibiotics( eg. Doxycycline).
SURGICAL MANAGEMENT-Surgical repair is recommended in patients. with asymptomatic aneurysm 5-5 cm in diameter or larger.
•Surgical procedure are
1)Open aneurysm repair (OAR)
2)Endovascular graft procedure
introduction,
definition
types
causes etc
Management
Routine ultrasound procedures. These procedures will monitor the size and rate of growth of the aneurysm every 6 months to 12 months as part of a "watchful waiting" approach for smaller aneurysms.
Controlling or modifying risk factors. Steps such as quitting smoking, controlling blood sugar if diabetic, losing weight if overweight or obese, and controlling dietary fat intake may help to control the progression of the aneurysm.
Medication. Medication can control factors such as hyperlipidemia (elevated levels of fats and cholesterol in the blood) and/or high blood pressure.
Surgery
Aneurysm open repair. An incision is made to directly visualize and repair the aneurysm. A cylinder-like tube called a graft may be used to repair the aneurysm. Grafts are made of various materials, such as Dacron The open repair is considered the surgical standard for an abdominal aortic aneurysm repair
Endovascular aneurysm repair (EVAR). EVAR is a procedure that requires only small incisions in the groin along with the use of X-ray guidance and specially-designed instruments to repair the aneurysm. With the use of special endovascular instruments and X-ray images for guidance, a stent-graft is inserted via the femoral artery and advanced up into the aorta to the site of the aneurysm.
ANEURYSMS , TYPES AND THERE MANAGEMENT.pptxBipul Thakur
Discussion about different types of Aneurysm, details about Abdominal aorta aneurysm and brief discussion about some important peripheral aneurysms.
Includes approach to different forms of Abdominal aortic aneurysm, its management and complications related to the surgery.
Chronic Stable Angina- Diagnosis & management
By Dr Awadhesh Kumar Sharma
Dr. Awadhesh kumar sharma is a young, diligent and dynamic interventional cardiologist. He did his graduation from GSVM Medical College Kanpur and MD in Internal Medicine from MLB Medical college jhansi. Then he did his superspecilisation degree DM in Cardiology from PGIMER & DR Ram Manoher Lohia Hospital Delhi. He had excellent academic record with Gold medal in MBBS,MD and first class in DM.He was also awarded chief ministers medal in 2009 for his academic excellence by former chief minister of UP Smt Mayawati in 2009.He is also receiver of GEMS international award.He had many national & international publications.He is also in editorial board of international journal- Journal of clinical medicine & research(JCMR).He is also active member of reviewer board of many journals.He is also trainee fellow of American college of cardiology. He is currently working in NABH Approved Gracian Superspeciality Hospital Mohali as Consultant Cardiologist.
Carotid artery disease is commonly seen in association with atherosclerosis and complicate the situation. clearcut guidelines with necessary surgical details are provided in presentations.
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
2. • An aneurysm is defined as a persistent, abnormal
dilatation of an artery to 1.5 times its normal diameter.
• A thoracic aortic aneurysm can involve the ascending aorta or
aortic root (60%), aortic arch (10%), descending aorta (40%), or
thoracoabdominal aorta (10%) segments*.
• Whilst thoracic aneurysms are less common than abdominal
aortic aneurysms, they are associated with high mortality.
They have an incidence of 6 in 100,000 person-years, with an
increasing prevalence with age.
3. Etiology
•
Thoracic aortic aneurysms develop due to degradation of the tunica media, the
layer of the artery which provides tensile strength and elasticity to the wall.
• As a result, the artery loses structural integrity and dilates, and as the
diameter increases, the wall tension rises and further increases the diameter in a
vicious cycle.
• The main causes of thoracic aneurysm are:
• Connective tissue diseases (e.g. Marfan’s syndrome or Ehlers-Danlos
syndrome)
• Bicuspid aortic valve
• Other causes include trauma, aortic dissection, aortic arteritis (e.g. Takayasu
Arteritis), and tertiary syphilis
• Thoracic aortic aneurysms grow at a mean rate of 1-2mm/year. This rate is higher
in those with Marfan’s syndrome, descending aneurysms (compared to
ascending aneurysms), and a dissected aneurysm (compared to a non-dissected
4. Risk factors
• The main risk factors for developing a thoracic aortic aneurysm
include family
history*, hypertension, atherosclerosis (specifically
descending aneurysms), smoking, high BMI, male
gender, and advancing age.
• *19% of patients have a positive family history
5. Clinical features
• Typically thoracic aneurysms are asymptomatic and are found
incidentally.
• In those that are symptomatic, the most common presenting
complaint is pain, with the location of the pain potentially
localising the aneurysm:
6. • Other symptoms of thoracic aneurysms include:
• Back pain – secondary to spinal compression by descending or
thoracoabdominal aneurysm
• Hoarse voice – from damage to the left recurrent laryngeal nerve in
arch aneurysms
• Distended neck veins – from SVC compression
• Symptoms of heart failure – from involvement of the aortic valve
• Dyspnoea or cough – secondary to tracheal or bronchial
compression
• Clinical signs are not commonly found on examination, however
chronic disease may present with the signs of aortic root disease or
heart failure.
• Thoracic aneurysms have a risk of rupture or dissection, which
are potentially lethal. An acute aortic syndrome will present
with sudden onset pain in the back, chest, neck, and/or abdomen
7. Differential diagnosis
• As thoracic aneurysms are mostly found incidentally on
imaging, other differential diagnosis are rarely considered
before the definitive diagnosis is determined.
• In symptomatic patients, the scope of symptoms for a thoracic
aneurysm is wide. However for those presenting with chest or
back pain (the most common presentation), diagnoses of ACS,
PE, pneumothorax, and aortic dissection should all be
considered.
8. Investigation
• Thoracic aneurysms are diagnosed through imaging. However, initial work-up should
include routine bloods (FBC, U&Es, clotting), an ECG, and a chest radiograph (CXR)
performed.
• Imaging
• Many thoracic aneurysms are first identified as incidental findings on imaging.
• A thoracic aneurysm can be seen on plain film chest radiograph demonstrating a
widened mediastinal silhouette, an enlarged aortic knob, and possible tracheal deviation
(Fig. 3). However, a radiograph is not sensitive enough to make the definitive diagnosis
and further imaging is required
• A CT chest scan with contrast is the preferred imaging modality for thoracic aneurysms,
providing sufficient detail to ascertain the level and the size of the aneurysm*.
• Transoesophageal echocardiography (TOE) can be used to good effect to further detect
any concurrent aortic insufficiency or dissection; TOE should form part of the routine
assessment of patients with Marfan’s disease and suspected thoracic aortic disease.
• *Due to the potentially tortuous nature of the thoracic aorta and the use of axial images in
CT scans, care must be taken to ensure the actual aortic diameter is being measured, not
simply measuring through the aorta off-axis; reconstructing axial imaging into 3D images via
CT angiography or MR angiography can overcome this issue
9. • Management
• Despite limited evidence, patients with a confirmed thoracic
aneurysm should be started on medical management,
alongside any concurrent further investigations and definitive
management planned.
• These patients are at increased cardiovascular risk, therefore
should be initiated on statin and anti-platelet therapy to
decrease the risk of myocardial infarction. Blood pressure
should be controlled and smoking cessation is imperative.
• Surgical Management
• Surgical management is dependent on the location of the
aneurysm, with the threshold for surgery varying according to
the health of the patient. Patients suffering from Marfan’s
syndrome or having a previous thoracic dissection have a
greater risk of dissection and rupture, and threshold levels for
intervention are often lower