Downloaded 143 times
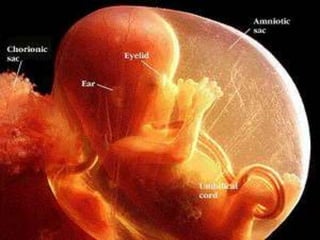

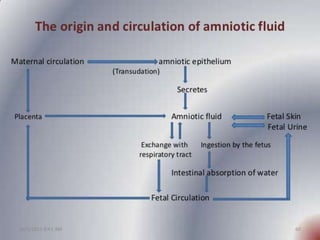
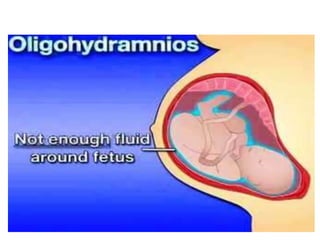



This document provides information about amniotic fluid development: - Amniotic fluid is contained within the amniotic sac and is derived from both maternal circulation and fetal parts. It is composed primarily of water but also contains small amounts of proteins, carbohydrates, lipids, electrolytes, and cells. - The volume of amniotic fluid increases throughout pregnancy, starting at around 30 ml at 10 weeks and reaching 800-1000 ml by 36-38 weeks. It is replaced every 3 hours through production from the amniotic membranes and fetal urine. - Amniotic fluid serves important functions like cushioning the fetus, maintaining temperature, and allowing freedom of movement. Analysis of amniotic fluid













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















