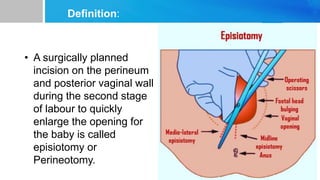
1. An episiotomy is a surgical incision made in the perineum and posterior vagina during childbirth to enlarge the vaginal opening for delivery.
2. While episiotomies were once routinely performed, evidence now supports a more restricted approach and performing them only when necessary to prevent tearing or aid delivery.
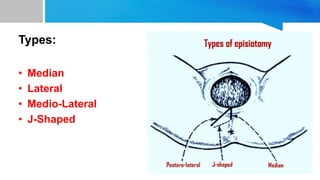
3. The main types of episiotomies are median, mediolateral, and lateral, with mediolateral being the most common. Structures that can be cut include the vaginal wall, perineal muscles, and fascia. Potential complications include bleeding, infection, pain during intercourse, and rare cases of rectal tissue or anal sphincter tearing




































































![Review of literature [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/reviewofliteratureautosaved-230315053854-fbe61789-thumbnail.jpg?width=640&height=640&fit=bounds)

![Bandages and Binders [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bandagesandbindersautosaved-230314063514-38348509-thumbnail.jpg?width=640&height=640&fit=bounds)



















